Chapter: Basic & Clinical Pharmacology : Pharmacologic Management of Parkinsonism & Other Movement Disorders
Monoamine Oxidase Inhibitors
MONOAMINE OXIDASE INHIBITORS
Two types of monoamine
oxidase have been distinguished in the nervous system. Monoamine oxidase A
metabolizes norepineph-rine, serotonin, and dopamine; monoamine oxidase B
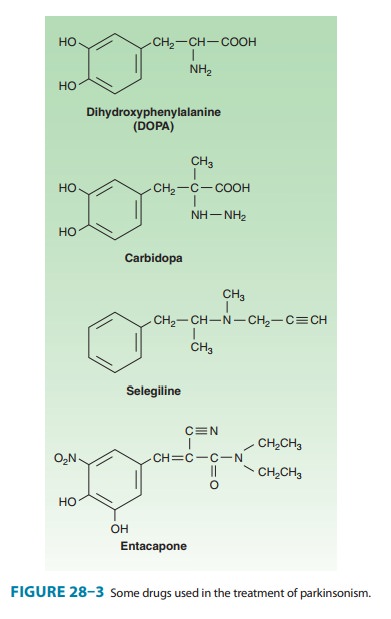
metabolizes dopamine selectively. Selegiline
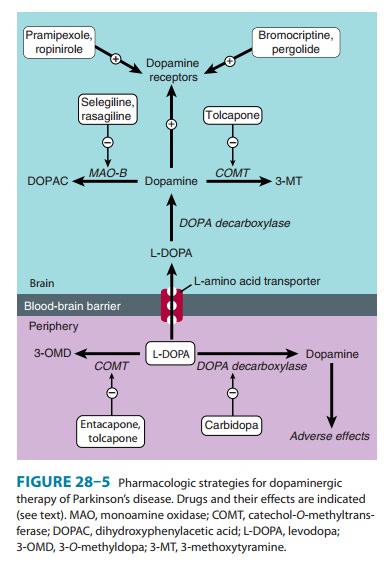
(deprenyl) (Figure 28–3), a selec-tive irreversible inhibitor of monoamine
oxidase B at normal doses (at higher doses it inhibits monoamine oxidase A as
well), retards the breakdown of dopamine (Figure 28–5); in consequence, it
enhances and prolongs the antiparkinsonism effect of levodopa (thereby allowing
the dose of levodopa to be reduced) and may reduce mild on-off or wearing-off
phenomena. It is therefore used as adjunctive therapy for patients with a
declining or fluctuating response to levodopa. The standard dose of selegiline
is 5 mg with breakfast and 5 mg with lunch. Selegiline may cause insomnia when
taken later during the day.
Selegiline has only a
minor therapeutic effect on parkin-sonism when given alone. Studies in animals
suggest that it may reduce disease progression, but trials to test the effect
of selegi-line on the progression of parkinsonism in humans have yielded
ambiguous results. The findings in a large multicenter study were taken to
suggest a beneficial effect in slowing disease pro-gression but may simply have
reflected a symptomatic response.
Rasagiline, another monoamine oxidase B inhibitor, is morepotent than
selegiline in preventing MPTP-induced parkinsonism and is being used for early
symptomatic treatment. The standard dosage is 1 mg/d. Rasagiline is also used
as adjunctive therapy at a dosage of 0.5 or 1 mg/d to prolong the effects of
levodopa-carbidopa in patients with advanced disease. A large double-blind,
placebo-controlled, delayed-start study (the ADAGIO trial) to evaluate whether
it had neuroprotective benefit (ie, slowed the disease course) yielded unclear
results: a daily dose of 1 mg met all the end points of the study and did seem
to slow disease progres-sion, but a 2-mg dose failed to do so. These findings
are difficult to explain and the decision to use rasagiline for neuroprotective
purposes therefore remains an individual one.
Neither selegiline nor
rasagiline should be taken by patients receiving meperidine, tramadol,
methadone, propoxyphene, cyclobenzaprine, or St. John’s wort. The antitussive
dextromethor-phan should also be avoided by patients taking one of the
mono-amine oxidase B inhibitors; indeed, it is wise to advise patients to avoid
all over-the-counter cold preparations. Rasagiline or selegi-line should be
used with care in patients receiving tricyclic antide-pressants or serotonin
reuptake inhibitors because of the theoretical risk of acute toxic interactions
of the serotonin syn-drome type , but this is rarely encountered in practice.
The adverse effects of levodopa may be increased by these drugs.
The combined
administration of levodopa and an inhibitor of both forms of monoamine oxidase
(ie, a nonselective inhibitor) must be avoided, because it may lead to
hypertensive crises, prob-ably because of the peripheral accumulation of
norepinephrine.
Related Topics