Chapter: Obstetrics and Gynecology: Abnormal Labor and Intrapartum Fetal Surveillance
Shoulder Dystocia
SHOULDER DYSTOCIA
Labor may sometimes arrest due to
shoulder dystocia. Shoulder dystocia cannot be predicted or prevented, be-cause
accurate methods for identifying which fetuses will experience this
complication do not exist. Antepartum conditions associated with shoulder
dystocia include multi-parity, postterm gestation, previous history of a
macro-somic birth, and a previous history of shoulder dystocia. Although fetal
macrosomia increases the risk of shoulder dystocia, elective induction of labor
or elective cesarean de-livery for all women suspected of carrying a fetus with
macrosomia is not appropriate.
Diagnosis of shoulder dystocia
has a subjective compo-nent, especially in less severe forms. The delivered
fetal head may retract against the maternal perineum (turtle sign) and, if so,
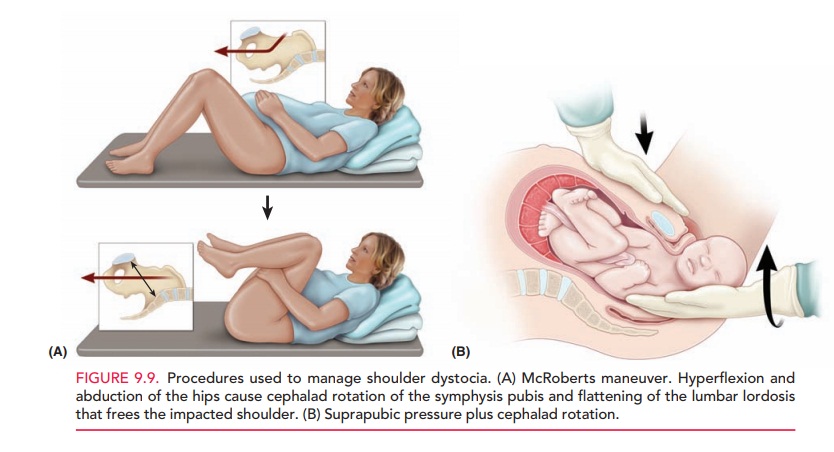
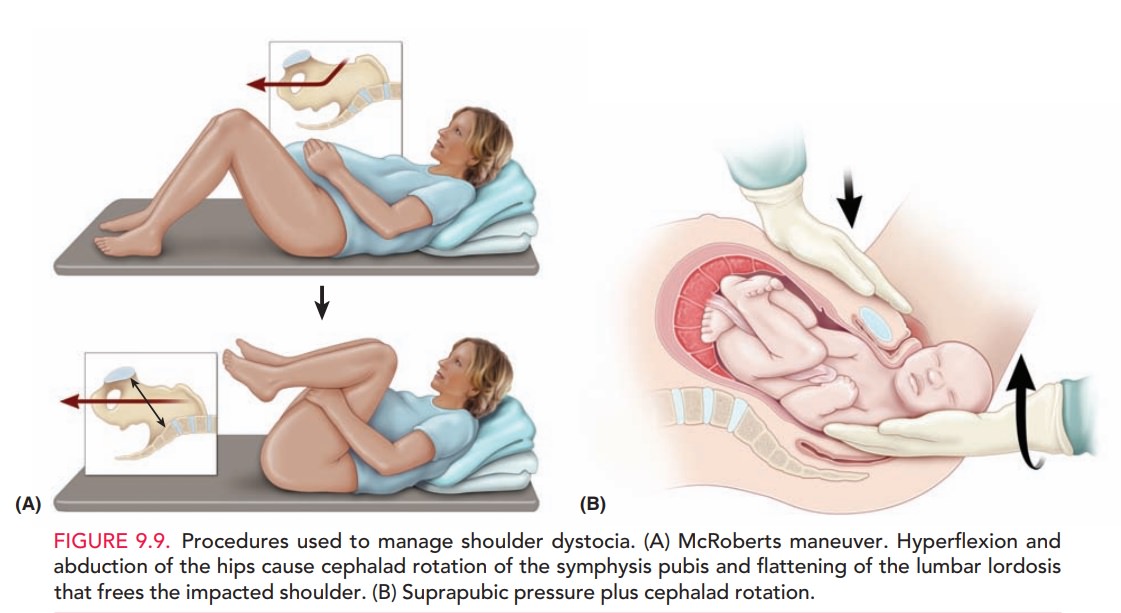
may assist in the diagnosis. Interventions that may be used to facilitate
delivery include the McRoberts maneu-ver and the application of suprapubic
pressure to assist in dislodging the impacted shoulder (Fig. 9.9). In contrast,
fundal pressure may further worsen impaction of the shoul-der and also may
result in uterine rupture. Controversy ex-ists as to whether episiotomy is
necessary, because shoulder dystocia typically is not caused by obstructing
soft tissue. Direct fetal manipulation with either rotational maneuvers or
delivery of the posterior arm also may be used. In severe cases, more
aggressive interventions, such as the Zavanelli maneuver (in which the fetal
head is flexed and reinserted into the vagina to reestablish umbilical cord
blood flow and delivery performed through fracture of the fetal clavicle, may
be performed. Regardless of the procedures used, brachial plexus injury is
associated with shoulder dystocia; incidence ranges from 4% to 40%. However,
most cases resolve without permanent disability; fewer than 10% of all cases of
shoulder dystocia result in a persistent brachial plexus injury.
Related Topics