Chapter: Obstetrics and Gynecology: Abnormal Labor and Intrapartum Fetal Surveillance
Diagnosis and Management of Abnormal Labor Patterns
Diagnosis and Management of
Abnormal Labor Patterns
Graphic documentation of
progressive cervical dilation and effacement facilitates assessing a patient’s
progress in labor and identifying abnormal labor patterns. The Friedman Curve
is commonly used for this purpose. Labor abnormalities can be categorized into
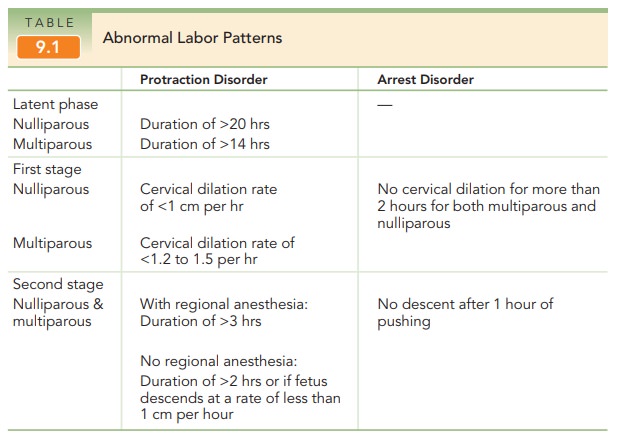
two general types: protraction disorders,
in which labor is slow to progress, and arrest
disorders, in which labor ceases to progress (Table 9.1). Protraction can
occur dur-ing both the latent and active phases of labor, while arrest is
recognized only in the active phase. Although the defi-nition of the latent phase of labor is controversial,
in gen-eral it can be defined as the phase in which the cervix effaces but
undergoes minimal dilation.
Management of abnormal labor
encompasses a wide range of options, from observation to operative or cesarean
delivery. Management choice depends on several factors:
·
Adequacy of uterine contractions
·
Fetal malposition or
cephalopelvic disproportion
·
Other clinical conditions, such
as nonreassuring fetal status or chorioamnionitis
Management decisions should be
balanced between ensur-ing a positive outcome for mother and fetus and avoiding
the concomitant risks of operative and cesarean delivery.
FIRST-STAGE DISORDERS
prolonged latent phase is one that exceeds 20 hours in
anulliparous patient or 14 hours in a multiparous patient. A pro-longed latent
phase does not necessarily predict an abnormal ac-tive phase of labor. Some
patients who have initially beendiagnosed as having a prolonged latent phase
are subse-quently found to have been in false labor. A prolonged la-tent phase
does not in itself pose a danger to the mother or fetus. Options for management
of women with a pro-longed latent phase of labor include observation and
seda-tion. With either of these options, the patient may stop having contractions,
in which case she is not in labor; may go into active labor; or may continue
experiencing pro-longed labor into the active phase. In the latter case, other
interventions as described below may be administered to augment uterine
contractions.
Once the patient is in active labor, the first stage is consid-ered prolonged when the cervix dilates less than 1 cm per hour in nulliparous women, and less than 1.2 to 1.5 cm per hour in multi-parous women. Management options for a prolonged firststage include observation, augmentation by amniotomy or oxytocin, and continuous support. Cesarean delivery usu-ally is warranted if maternal or fetal status becomes non-reassuring.
Augmentation Augmentationrefers to stimulation ofuterine contractions when spontaneous
contractions have failed to result in progressive cervical dilation or de-scent
of the fetus. Augmentation can be achieved with amniotomy (artificial rupture of membranes) or oxy-tocin
administration. Augmentation should be
consideredif the frequency of contractions is less than 3 contractions per 10
minutes or the intensity of contractions is less than 25 mm Hg above the
baseline or both. Before augmentation, the mater-nal pelvis and cervix as
well as fetal position, station, and well-being should be assessed. If there is
no evidence of disproportion, oxytocin can be used if uterine contractions are
judged to be inadequate. Contraindications to aug-mentation are similar to
those for labor induction .
If the
membranes have not ruptured, amniotomy may en-hance progress in the active
phase and negate the need for oxytocin augmentation. Amniotomy
allows the fetal head, rather thanthe otherwise intact amniotic sac, to be the
dilating force. It may also stimulate the release of prostaglandins, which
could aid in augmenting the force of contractions.
Amniotomy is usually performed
with a thin, plastic rod with a sharp hook on the end. The end is guided to the
open cervical os with the examiner’s fingers, and the hook is used to snag and
disrupt the amniotic sac. Risks of amniotomy include fetal heart rate
decelerations due to cord compression and an increased incidence of
chorioamnionitis. For these reasons, amniotomy should not be routine and should
be used for women with pro-longed labor. The fetal heart rate (FHR) should be
eval-uated both before and immediately after rupture of the membranes.
It has
been shown that amniotomy combined with oxytocin administration early in the
active stage reduces labor by up to 2 hours, although there is no change in the
rate of cesarean delivery with this treatment protocol.
The goal of oxytocin
administration is to effect uterine ac-tivity sufficient to produce cervical
change and fetal de-scent while avoiding uterine hyperstimulation and fetal
compromise. Typically, a goal of a maximum of 5 contrac-tions in a 10-minute
period with resultant cervical dilation is considered adequate. Oxytocin may be
administered in low-dose or high-dose regimens. Low-dose regimens are associated
with a decreased incidence and severity of uterine hyperstimulation. High-dose
regimens are associated with decreased labor times, incidence of
chorioamnionitis, and cesarean delivery for dystocia.
Continuous Labor
Support Continuous support duringlabor from
caregivers (nurses, midwives, or lay individuals) may have a number of benefits
for women and their new-borns. Continuous care has been associated with reduced need for
pain relief and oxytocin administration, lower rates of cesarean and operative
deliveries, decreased incidence of 5-minute Apgar scores lower than 7, and
increased patient satisfaction with the labor experience. However, there are
insufficient data comparing differences in benefits on the basis of level of
training of support personnel—that is, whether the caregivers were nurses,
midwives, or doulas. There is no evidence of harmful effects from continuous
support during labor.
SECOND-STAGE DISORDERS
A
second-stage protraction disorder should be considered when the second stage
exceeds 3 hours if regional anesthesia has been ad-ministered, or 2 hours if no
regional anesthesia is used, or if the fetus descends at a rate of less than 1
cm per hour if no regional anesthesia is used. Second-stage arrest is diagnosed
when there is no descent after 1 hour of pushing. In the
past, the fetus wasthought to be at increased risk for morbidity and mortality
when the second stage exceeded 2 hours. Currently, more intensive intrapartum
surveillance provides the ability to identify the fetus that may not be
tolerating labor well.
Thus, the
length of the second stage of labor is not in itself an absolute or even a
strong indication for operative or cesarean delivery.
As long as heart tones continue
to be reassuring and cephalopelvic disproportion has been ruled out, it is
con-sidered safe to allow the second stage to continue. If uterine contractions
are inadequate, oxytocin adminis-tration can be initiated or the dosage
increased if already in place.
Bearing down efforts by the
patient in conjunction with uterine contractions help bring about delivery.
Labor positions other than the dorsal lithotomy position (e.g., knee-chest,
sitting, squatting, or birth-chair) may bring about subtle changes in fetal
presentation and facilitate vaginal delivery. Fetal accommodation may also be
facili-tated by allowing the effects of epidural analgesia to dissi-pate. The
absence of epidural analgesia may increase the tone of the pelvic floor
muscles, facilitating the cardinal movements of labor and restoring the urge to
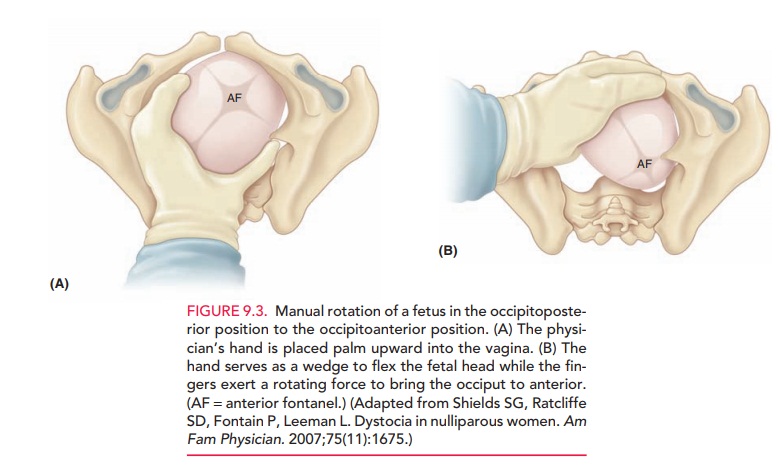
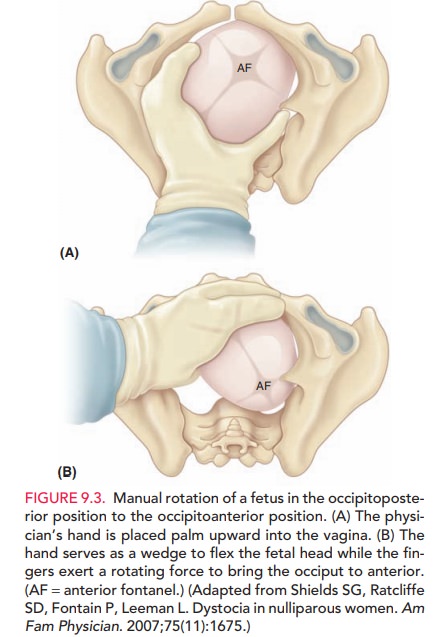
push. In some cases of fetal malpresentation, manual techniques can facilitate
delivery. If the fetus is in the occipitoposte-rior position and does not
spontaneously convert to the nor-mal position, rotation can be performed to
turn the fetus to the anterior position (Fig. 9.3).
The decision to perform an
operative delivery in the second stage versus continued observation should be
made on the basis of clinical assessment of the woman and the fetus and the
skill and training of the obstetrician. Nonreassuring status of the fetus or
mother is an indica-tion for operative or cesarean delivery.
Related Topics