Chapter: Obstetrics and Gynecology: Abnormal Labor and Intrapartum Fetal Surveillance
Factors That Contribute to Normal Labor - The Three Ps
Factors That Contribute to Normal
Labor— The Three Ps
Labor is the
occurrence of uterine contractions of suffi-cient intensity, frequency, and
duration to bring about demonstrable effacement and dilation of the cervix. Dystocia
results from what have been categorized classi-cally as abnormalities of the
“power” (uterine contractions or maternal expulsive forces), “passenger”
(position, size, or presentation of the fetus), or “passage” (pelvis or soft
tissues).
UTERINE CONTRACTIONS (“POWER”)
Uterine
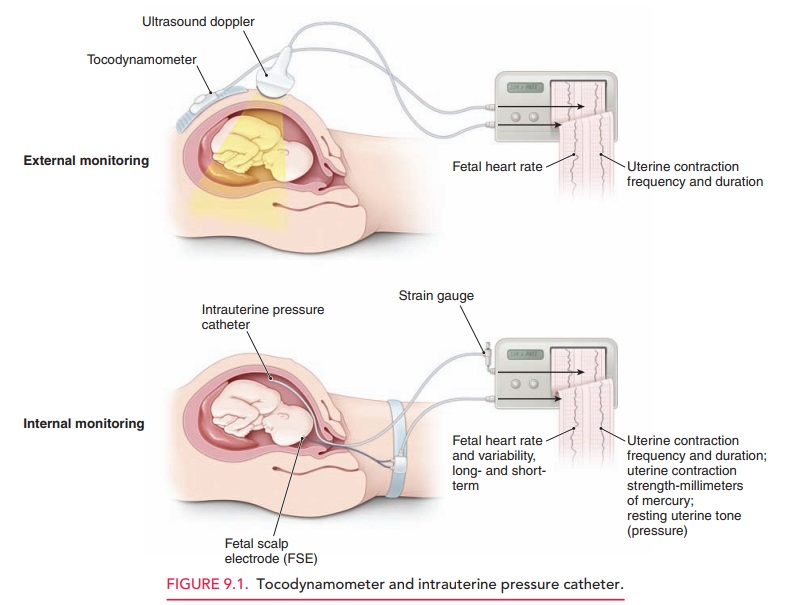
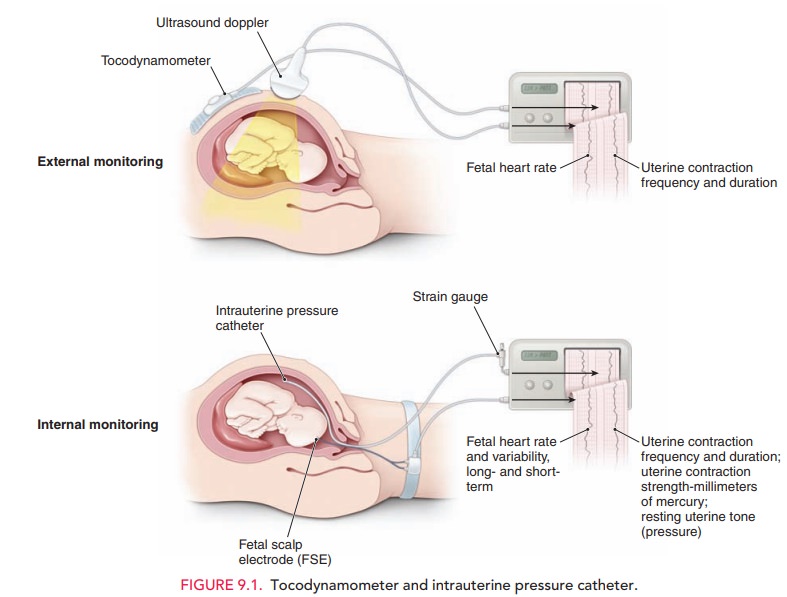
activity can be monitored by palpation, external tocody-namometry, or by using
intrauterine pressure catheters (IUPCs) (Fig.
9.1). A tocodynamometer is an external strain gauge that is placed on the
maternal abdomen. It records the frequency of uterine contractions and
relaxations, as well as the duration of each contraction. An IUPC, in ad-dition
to recording contraction frequency and duration, also directly measures the
pressure generated by uterine contractions, via a catheter inserted into the
uterine cav-ity. The catheter is attached to a gauge that measures
intra-uterine pressure in millimeters of mercury (mm Hg).
Recent
studies suggest that the use of an IUPC instead of external tocodynamometry
does not affect the outcome in cases of abnormal labor.
However, an IUPC may be useful in
specific situations, such as maternal obesity or other factors that may prevent
accurate clinical evaluation of uterine contractions.
For cervical dilation and fetal descent to occur, each uterine contraction must generate at least 25 mm Hg of peak pressure. Optimal intrauterine pressure is 50 to 60 mm Hg. The frequency of uterine contractions is also impor-tant in generating a normal labor pattern: the optimal fre-quency of uterine contractions is a minimum of three contractions in a 10-minute interval, often described as “adequate.” Uterine contractions that are too frequent are not optimal, because they prevent intervals of uterine re-laxation. During this “rest interval,” the fetus receives unimpeded uteroplacental blood flow for oxygen and waste transport. Without these rest periods, fetal oxygenation may be compromised.
Another unit of measure commonly
used to assess con-tractile strength is the Montevideo unit (MVU). This unit is the number of uterine
contractions in 10 minutes times the average intensity (above the resting
baseline intrauterine pressure). Normal
progress of labor is usually associated with 200or more Montevideo units.
FETAL FACTORS (“PASSENGER”)
Evaluation of the passenger
includes clinical estimation of fetal weight and clinical evaluation of fetal
lie, presenta-tion, position, and attitude. If
a fetus has an estimated weightgreater than 4000 to 4500 grams, the risk of
dystocia, includ-ing shoulder dystocia and fetopelvic disproportion, is
greater. Because ultrasound estimation of fetal weight is often in-accurate
by as much as 500 to 1000 grams when the fetus is near term (40 weeks’
gestational age), this information must be used in conjunction with other
parameters when making management decisions.
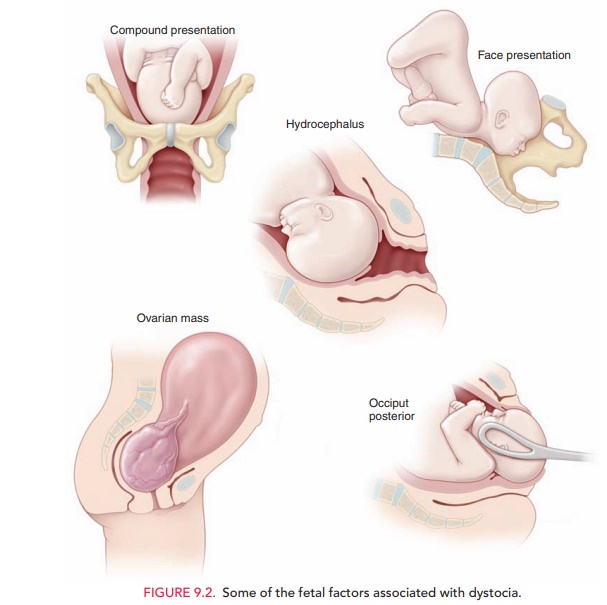
Fetal
attitude, presentation, and lie also play a role in the progress of labor (Fig.
9.2). If the fetal head is asynclitic (turnedto one side; asynclitism) or extended (extension),
a larger cephalic diameter is presented to the pelvis, thereby increas-ing the
possibility of dystocia. A brow
presentation (about 1 in 3000 deliveries) typically converts to either a
vertex or face presentation, but, if persistent, may cause dystocia re-quiring
cesarean delivery. Likewise, a face
presentation (about 1 in 600 to 1000 deliveries) requires cesarean
deliv-ery in most cases. However, a mentum
anterior presenta-tion (chin toward mother’s abdomen) may be
deliveredvaginally if the fetal head undergoes flexion, rather than the normal
extension. A persistentoccipitoposterior positionis
alsoassociated with longer labors (approximately 1 hour in multiparous patients
and 2 hours in nulliparous patients). Incompoundpresentations, when one or more limbs prolapse alongsidethe
presenting part (about 1 in 700 deliveries), the extrem-ity usually retracts
(either spontaneously or with manual as-sistance) as labor continues. When it
does not, or in the 15% to 20% of compound presentations associated with
umbili-cal cord prolapse, cesarean delivery is required.
Fetal anomalies, such as hydrocephaly and soft tissue tumors, may also cause dystocia. The routine use of prena-tal ultrasound for other causes has allowed identification of these situations, significantly reducing the incidence of un-expected dystocia of this kind.
MATERNAL FACTORS (“PASSAGE”)
A number of maternal factors are
associated with dystocia. Dystocia can result from maternal skeletal or
soft-tissue anomalies that obstruct the birth canal. Cephalopelvicdisproportion, in which the size of the maternal
pelvis isinadequate to the size of the presenting part of the fetus, may impede
fetal descent into the birth canal.
Clinical,
radiographic, and CT measurements of the bony pelvis are poor predictors of
successful vaginal delivery, due to the inaccuracy of these measurements as
well as case-by-case differences in fetal accommodation and mechanisms of
labor.
Clinical
pelvimetry, the manual evaluation of the diam-eters of the
pelvis, is also a poor predictor of successful vaginal birth, except in rare
circumstances when the pelvic diameters are so small as to render the pelvis
“completely contracted.” Although radiographic and CT pelvimetry can be helpful
in some cases, the progress of descent of the presenting part in labor is the
best test of pelvic adequacy.
Soft-tissue causes of dystocia
include abnormalities of the cervix, tumors or other lesions of the colon or
adnexa, distended bladder, uterine fibroids, an accessory uterine horn, and
morbid obesity. Epidural anesthesia may con-tribute to dystocia by decreasing
the tone of the pelvic floor musculature.
Risks
Dystocia
may be associated with serious complications for both the woman and the fetus. Infection
(chorioamnionitis) is aconsequence of prolonged labor, especially in the
setting of ruptured membranes. Fetal infection and bacteremia, including
pneumonia caused by aspiration of infected amniotic fluid, is linked to
prolonged labor. In addition, there are the attendant risks of cesarean or
operative de-livery, such as maternal soft tissue injury to the lower genital
tract and fetal trauma
Related Topics