Chapter: Surgical Pathology Dissection : The Digestive System
Polypectomies - Neoplastic Intestinal Disease: Surgical Pathology Dissection
Neoplastic Intestinal Disease
Polypectomies
Polyps
of the gastrointestinal tract are usually removed endoscopically by a single
incision at the base of the polyp stalk. Although these speci-mens lack the
size and complexity of more extended bowel resections, they are delicate
structures that require meticulous processing. First, obtain relevant clinical
information such as the patient’s history, the endoscopic findings, and the
anatomic site from which the polyp was re-moved. Next, turn your attention to
the specimen itself. The polypectomy specimen poses three important questions
to the surgical pathologist:
Are
adenomatous changes present? (2) Is in-filtrating carcinoma present, and if it
is does it infiltrate into the stalk? (3) Do any of the neoplas-tic changes
extend to the resection margin at the base of the stalk? Clearly, the
polypectomy speci-men must be carefully oriented and processed so that these
issues can be addressed.
The key
to orienting the polyp is to find its stalk. This may require careful
inspection, since a short stalk is often overshadowed by the much larger head
of the polyp. After finding the stalk, mark its base (i.e., the resection
margin) with either ink or colored tattoo powder. Measure the height and
diameter of the polyp. Next, place the speci-men in formalin for fixation.
Given the soft and spongy consistency of the fresh polyp, sectioning the polyp
is greatly facilitated if it is well fixed.
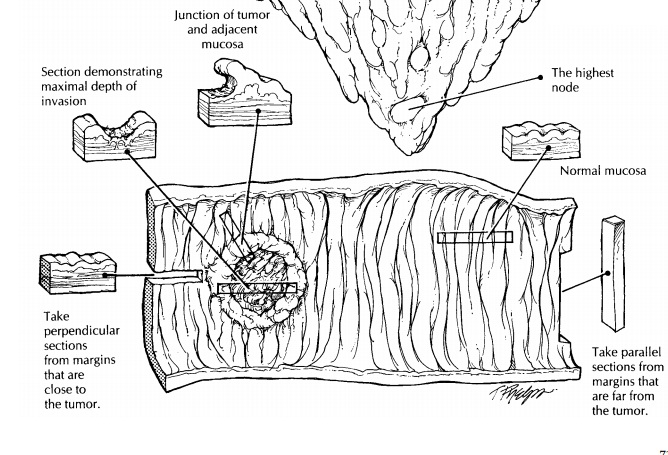
Once
fixed, the specimen should be sectioned in a way to show the relationship of
the stalk to the head of the polyp. As illustrated, this relation-ship is
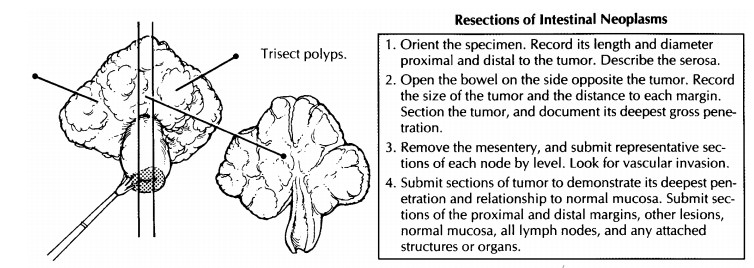
usually best demonstrated by trisecting the polyp into two lateral caps and one
median section that includes the stalk and the center of the head. The median
section should demonstrate the largest cross-sectional area of the head of the
polyp, its interface with the stalk, and the surgical margin. The importance of
trisecting the polyp is readily apparent if one pauses to consider the impact
of this method on the his-tologic sections. Serial sections into the median
section of a trisected polyp will approach the point of interest, the center of
the polyp. To avoid missing a small focus of carcinoma, submit the entire
specimen for histologic evaluation.
Important Issues to Address in Your Surgical Pathology Report on Polyps
·
What procedure was performed, and what
structures/organs are present?
·
What is the histologic type of the polyp (e.g.,
adenomatous, hyperplastic, hamartomatous, inflammatory)?
·
For adenomatous polyps, is the polyp
architec-turally tubular, villous, or tubulovillous?
·
If a carcinoma is present, what is the depth of
invasion of the tumor? (Specify the presence or absence of invasion of the
stalk and of the submucosa at the base of the stalk or base of a sessile
polyp.) Specify whether there are any poorly differentiated areas.
·
Is there evidence of vascular invasion?
·
What is the status of the resection margin at
the base? Measure (in millimeters) the distance from the deepest part of the
invasive carcinoma component to the nearest polyp margin. Does the adenomatous
epithelium or the infiltrating carcinoma extend to this margin?
Related Topics