Chapter: Surgical Pathology Dissection : The Digestive System
Cholecystectomies: Surgical Pathology Dissection
Cholecystectomies
The
gallbladder is one of the more frequently encountered specimens in the surgical
pathol-ogy laboratory. It is usually removed for stones and/or an inflammatory
condition, but it rarely does harbor a neoplasm.
The
gallbladder is a saccular structure com-posed of a fundus, body, and neck. It
progres-sively narrows to form the cystic duct. Even though this structural
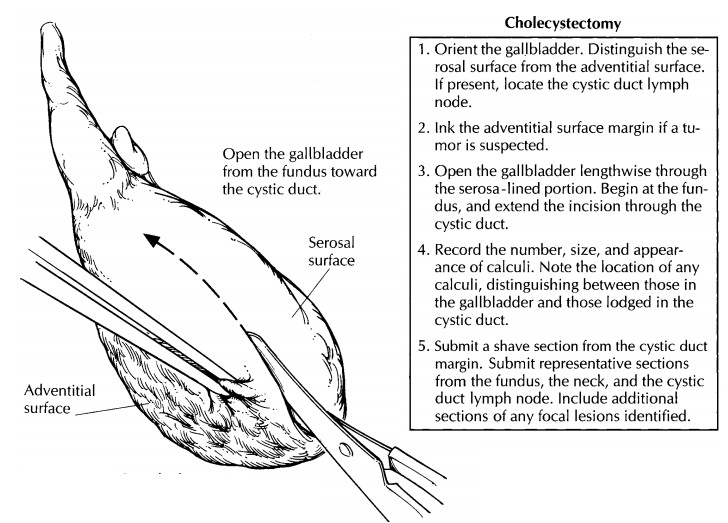
anatomy is straightfor-ward, take a moment to orient the specimen and identify
a few important features. First, note that the usual gallbladder has two very
different ex-ternal surfaces. One side of the gallbladder is smooth and glistening,
whereas the other is rough. The distinction between these two surfaces is
important. The smooth surface is lined by perito-neum. In contrast, the rough
surface is where the adventitia of the gallbladder has been dissected from the
undersurface of the liver, and it re-presents a surgical margin. (Rarely, a
gallbladder is entirely buried within the liver parenchyma or is attached to
the liver only by a mesentery.) Second, the lymphatics of the gallbladder drain
into a lymph node located along the cystic duct. When present in the specimen,
this cystic duct lymph node can be identified by palpating the soft tissues
investing the cystic duct.
State whether the gallbladder is received fresh or in fixative. Measure the specimen, and describe the external surfaces. One important issue to address at the onset of the dissection is whether the specimen is received intact. Not uncommonly, a gallbladder is opened in the operating room and the stones removed. Receipt of a previously opened gallbladder should be documented in the gross description. If the specimen is still in-tact, open the gallbladder lengthwise through its serosa-lined surface. Using a small pair of scissors, begin at the fundus; next, extend the cut through the body and neck of the gallbladder and then through the cystic duct. The lumen of the cystic duct should be examined, even though the duct may be tortuous and difficult to open. The direction in which the gallbladder is opened is important. Do not begin at the opening of the cystic duct because a probe or scissors forced into this opening could dislodge stones.
After
the specimen has been opened, note the contents of the gallbladder and the
cystic duct. Is the usual thin, dark green bile present; or is it hemorrhagic,
viscous, or sludgy? Is the lumen filled with pus (an infected gallbladder) or
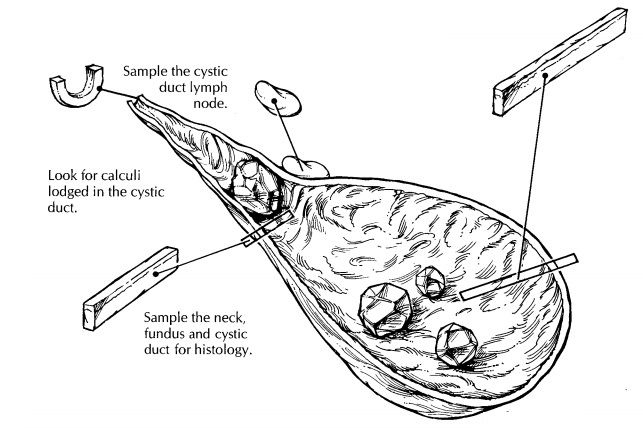
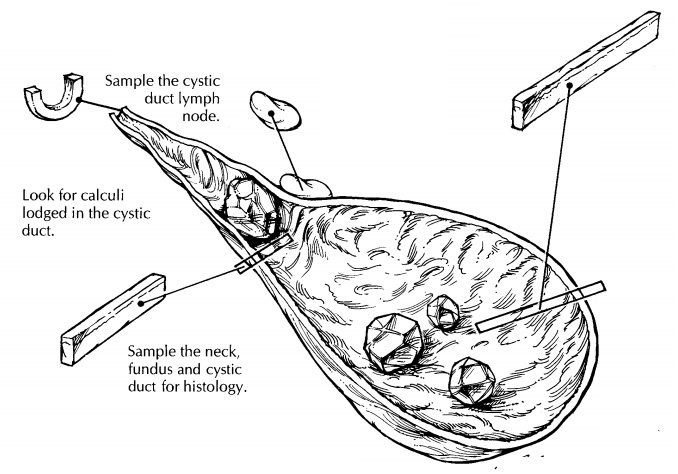
re-placed by clear white mucoid material (muco-cele)? Look for calculi, and
determine whether they are present within the lumen of the gallblad-der or
within the cystic duct. Record the appear-ance of any calculi. Are they round
or faceted? What is their color? Use a sharp blade to cut the calculi in half,
and note the appearance of their cut surfaces. How many calculi are present?
When numerous calculi are present, there is a tendency to record the size of
the largest one. In-stead, record the full range of sizes, keeping in mind that
the smaller calculi are more apt to become lodged in the cystic duct than are
the larger ones.
Next,
measure the thickness of the gallbladder wall, and describe the appearance of
the mucosa. The mucosa is normally bile-stained and has a fine, honeycombed
appearance. A frequent mucosal abnormality is cholesterolosis, in which there
are numerous yellow punctate deposits or interlacing linear yellow streaks on
the mucosa (“strawberry gallbladder”). If a neoplasm is sug-gested by the
presence of an exophytic or ulcera-tive lesion, the external adventitial
surface should be inked, as it represents an important surgical margin.
Describe the location of the neoplasm, its dimensions, and its configuration
(e.g., exo-phytic, ulcerating, diffusely infiltrating with as-sociated wall
thickening). If liver parenchyma is attached to the adventitial surface of the
gall-bladder, does the tumor appear to invade the liver?
The
gallbladder is best sampled after it has been allowed to fix. For routine
specimens, submit one representative full-thickness section from the fundus,
one through the body/neck of the gallbladder, and one cross section of the
cystic duct margin. Additional sections are required when focal lesions are
present. If a neoplastic process is suspected, obtain full-thickness sec-tions
of the tumor to demonstrate its maximum depth of invasion. Also submit sections
from the periphery of the tumor to demonstrate its relationship to the
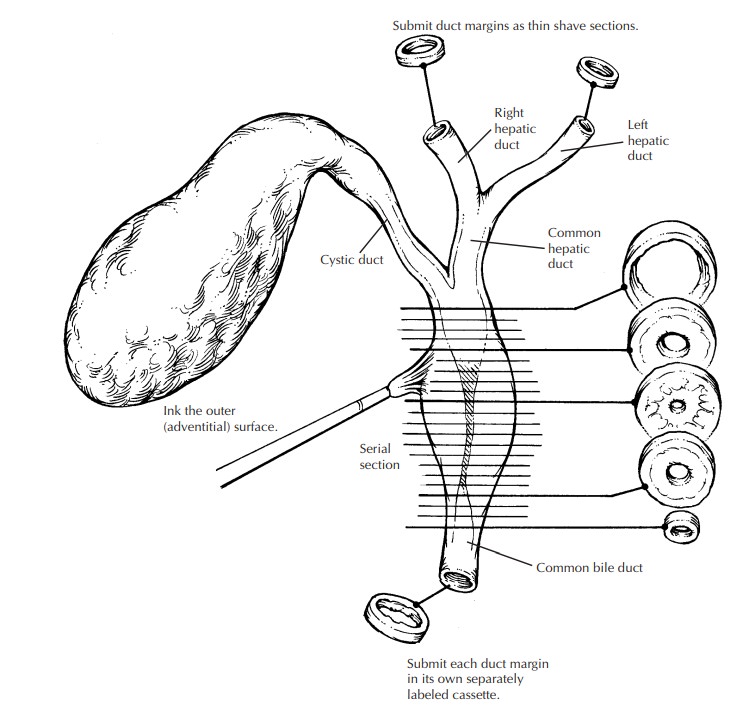
surrounding uninvolved mucosa. To assess the status of the margins when a
neoplasm is suspected, submit a shave section from the cystic duct margin and
perpendicular sections from the inked adventitial surface. When present, the
cystic duct lymph node should always be submitted for histologic evaluation.
Related Topics