Chapter: Surgical Pathology Dissection : The Digestive System
Liver Explants: Surgical Pathology Dissection
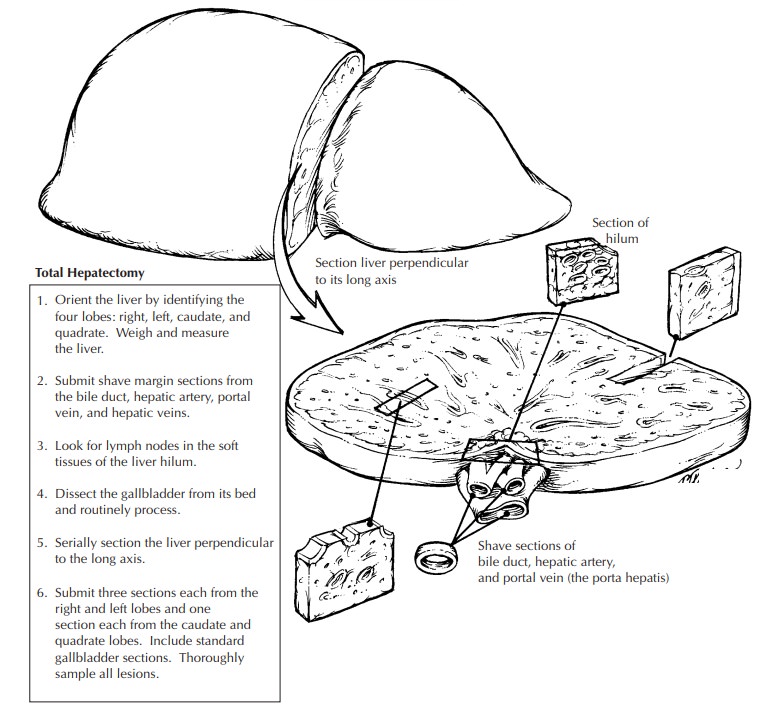
Liver Explants
Entire
liver resections are encountered in hospi-tals where liver transplantations are
performed.
The aim
of these dissections is to document the cause of the patient’s hepatic failure
and, in the cases of liver tumors, to stage the tumor and assess the margins at
the porta hepatis. Not infrequently, the cause of the hepatic failure is
infectious. Be very careful in handling these specimens, and as always strictly
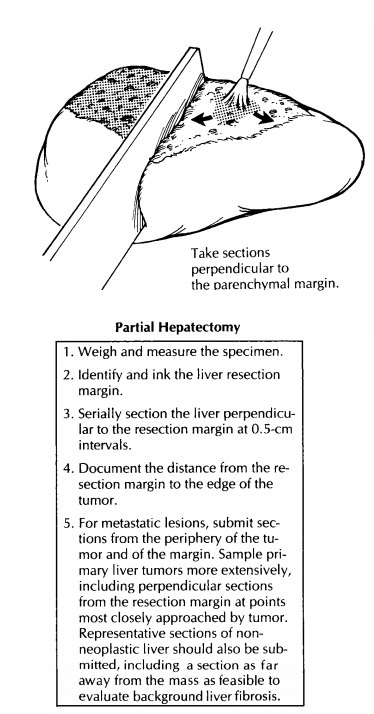
observe univer-sal precautions. It is not unreasonable to take the margins,
thinly section the specimen (see figure), and submerge the entire specimen in
formalin before further processing.
To
sample all regions of the liver adequately and to evaluate the important
structures of the porta hepatis, you will need to remember the basic anatomy of
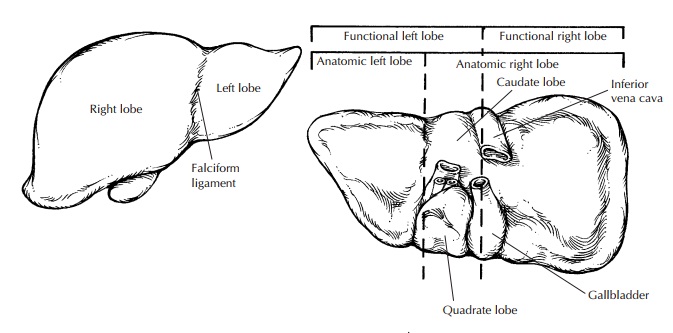
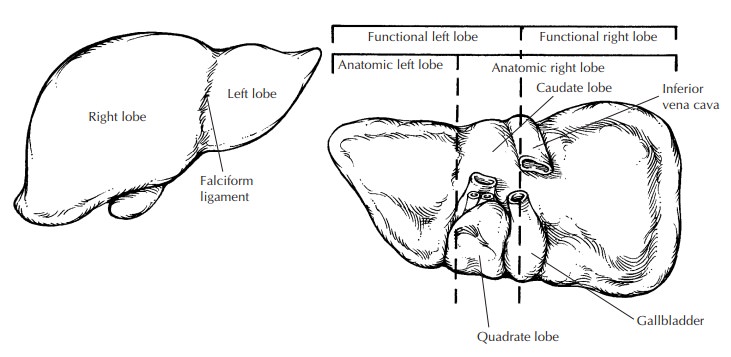
the liver. As illustrated, the liver is made up of four lobes. Viewed from
above, the anatomic right and left lobes are separated by the falciform
ligament. The two central lobes are best appreciated by examining the
undersur-face of the liver. The caudate lobe sits between the portal vein and
the inferior vena cava. The quadrate lobe is between the gallbladder fossa and
the ligamentum teres and is separated from the caudate lobe by the portal vein.
Sometimes the liver is more simply divided into functional right and left lobes
by a plane that passes from the gallbladder bed through the inferior vena cava.
The major structures forming the porta hepatis are the bile duct, hepatic
artery, and portal vein. These three structures maintain a con-sistent
relationship one to another. The duct is most anterior and to the right, the
artery is to the left, and the vein is most posterior.
Weigh
and measure the liver, and record the appearance of its external surface. If
the gallblad-der is present, record its size as well. Begin the dissection at
the liver hilum. Avoid the tempta-tion to section the liver parenchyma before
the hilar structures have been located, identified, and sampled. First,
identify and submit a shave sec-tion (complete cross section) of the common
he-patic duct, the hepatic artery, the portal vein, and hepatic veins.
Typically, the hilar vessels and bile duct have been surgically clipped or
sutured by the surgeon and can thus be easily located. The portal vein and
hepatic veins are frequently tran-sected quite close to the liver, with little
extrahe-patic tissue remaining. In these cases, the margins may have to be of
the initial intrahepatic portion of these vessels. Remember to check for
throm-boemboli. In cases of chronic extrahepatic bili-ary tract disease, the
extrahepatic bile duct may be difficult to recognize. If this is the case, make
a cut in the liver parallel to the porta hep-atis, about 1 cm away from the
porta hepatis. Now locate a large bile duct (by its green-yellow color) and
insert a probe back toward the porta hepatis to reveal the extrahepatic bile
duct. Look for lymph nodes in the hilar soft tissues, and sample each of these
for histologic evaluation. Take a section perpendicular to the hilum that
captures the soft tissue of the porta hepatis and the underlying liver. This
section provides a look at many larger bile ducts and peribiliary glands. Next,
dissect the gallbladder from its bed, and process it as you would a routine
cholecystec-tomy.
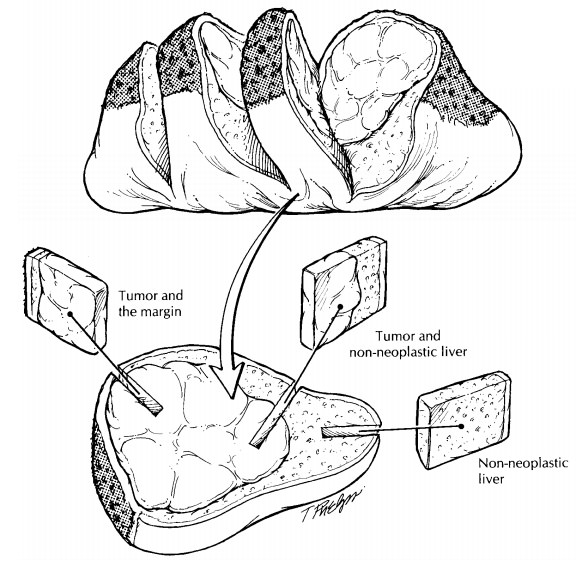
Now that
the porta hepatis has been carefully examined and sampled, section the liver
par-enchyma. Using a long, sharp knife, section the liver as illustrated.
Record the color and consis-tency of the liver parenchyma. Is the liver
nodu-lar, fibrotic, or necrotic? Are any focal lesions present?
In
addition to the sections taken of the porta hepatis, all lobes of the liver
should be repre-sented in a routine sampling of the explanted liver. Three
sections each from the right and left lobes and one section each from the
caudate
and
quadrate lobes are generally sufficient, but more sections may be required to
sample all areas that have a distinct appearance. Additional sec-tions should
also be taken of any focal lesions.
Important Issues to Address in Your Surgical Pathology Report on Liver Explants
·
What procedure was performed, and what
structures/organs are present? How much does the liver weigh?
·
What are the nature and extent of the disease
that underlies the liver failure?
·
Are there any thromboemboli in large vessels?
·
Is the gallbladder present? Are calculi or any
other pathologic processes identified?
·
Is a neoplasm present? What are its type,
grade, size, and location? Does the tumor involve the structures of the porta
hepatis? Are the margins at the porta hepatis involved by tumor?
·
How many lymph nodes were examined, and how
many of them harbor a metastasis?
Related Topics