Chapter: Surgical Pathology Dissection : The Digestive System
Liver: Surgical Pathology Dissection
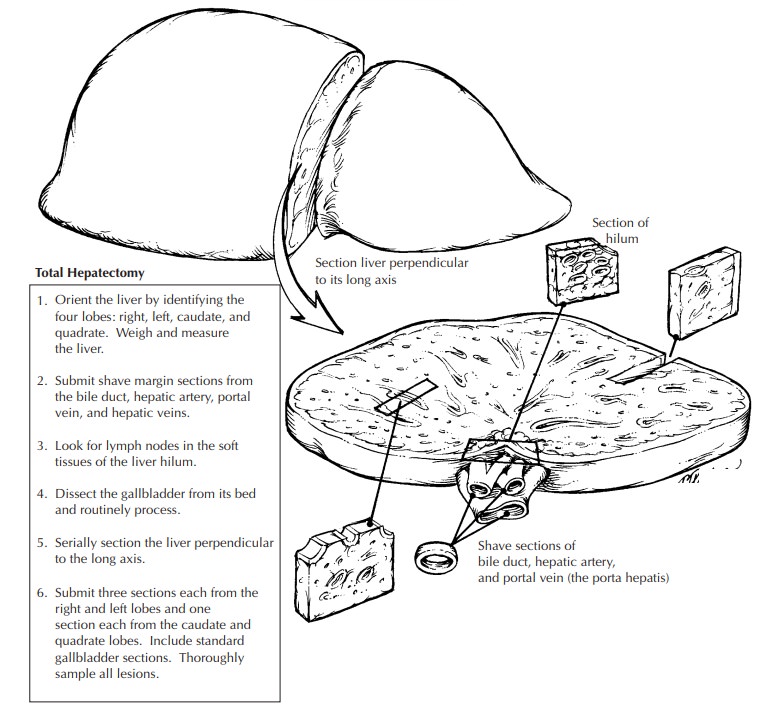
Liver
Biopsies
Biopsies
of the liver come in two forms: the deli-cate needle-core biopsy and the larger
wedge biopsy. In either case, the specimen should be measured and submitted in
its entirety for rou-tine histology. Thin-core biopsies are particularly
susceptible to desiccation. Therefore, unless special studies are indicated,
biopsies should be placed in fixative in the operating room. The core biopsy
can be embedded whole, while the wedge biopsy may be thick enough to warrant
sectioning before submitting to the histology lab-oratory. When sectioning the
wedge biopsy, iden-tify the smooth capsule, and then cut the liver at 0.2-cm
intervals perpendicular to this surface. Multiple slides should be prepared
from each tissue block for histologic evaluation. Step sec-tions are preferred
to serial sections so that the intervening sections are available for special
stains. If a storage disease is suspected, then a small portion of the biopsy
should be placed in glutaraldehyde for electron microscopy.
Partial Hepatectomy
Focal
lesions in the liver can be removed by par-tial liver resections. The extent of
these resections varies from small wedges to the removal of an entire lobe.
Regardless of its size, the partial liver resection is not structurally complex.
Typically, it consists of a focal lesion surrounded by a vari-able rim of
non-neoplastic liver parenchyma. Several faces of the specimen are covered by a
peritoneal lining, but at least one surface shows exposed hepatic parenchyma.
This exposed sur-face is the surgical resection margin. This mar-gin has to be
correctly identified and oriented. Identification of the resection margin is
seldom problematic. Unlike the smooth contour of the peritoneal-lined liver
capsule, the resection plane exposes liver parenchyma—which may be fragmented
or bloody—and shows cautery effect. On the other hand, orientation of the
margin can be very difficult, given the paucity of anatomic landmarks in these
limited resections. If the surgeon needs to know the precise location at which
a tumor involves or approaches the surgi-cal margin, orientation will require
the surgeon’s assistance.
Once the
margin is identified and the specimen oriented, weigh the specimen, and measure
it in each dimension. Examine its contours and sur-faces. A bulge in the
surface of the liver and/ or retraction of the serosa can help localize an
intraparenchymal mass. Livers resected for trau-matic ruptures should be
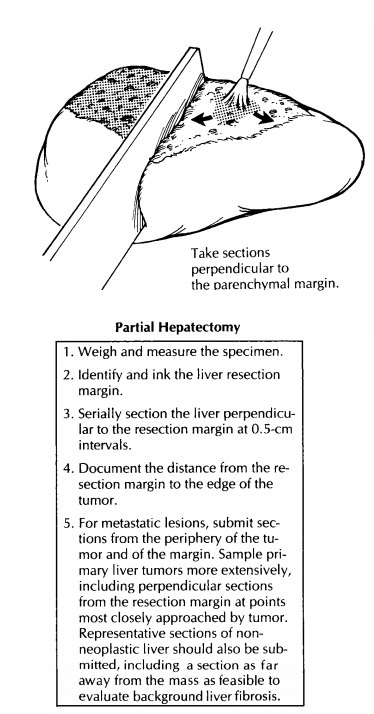
carefully examined for lacerations of the capsule. Next, rinse the blood from
the cut margin, blot it with paper towels, and then ink the dry resection
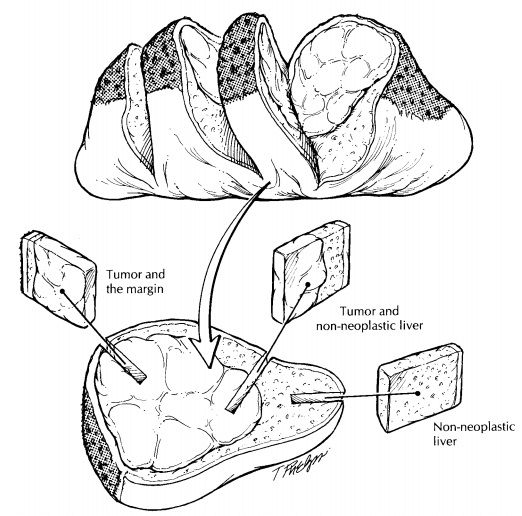
margin. As il-lustrated, serially section the liver perpendicular to the
resection margin. The initial section should pass through the center of the
tumor to demon-strate the closest approach of the tumor to the resection
margin. Continue sectioning the liver parallel to this first cut at thin (e.g.,
0.5-cm) in-tervals. Examine all cut surfaces for additional nodules.
Record the number, size, location, color, consis-tency, and circumscription of all lesions. Note the presence or absence of necrosis, hemorrhage, and scarring. Measure the distance from all lesions to the surgical resection margin. If intrahepatic blood vessels are apparent, examine them for tumor thrombi. Remember to describe the appear-ance of the non-neoplastic hepatic parenchyma. Is the lesion arising in a background of cirrhosis? Is there intraparenchymal hemorrhage associated with an overlying laceration of the capsule?
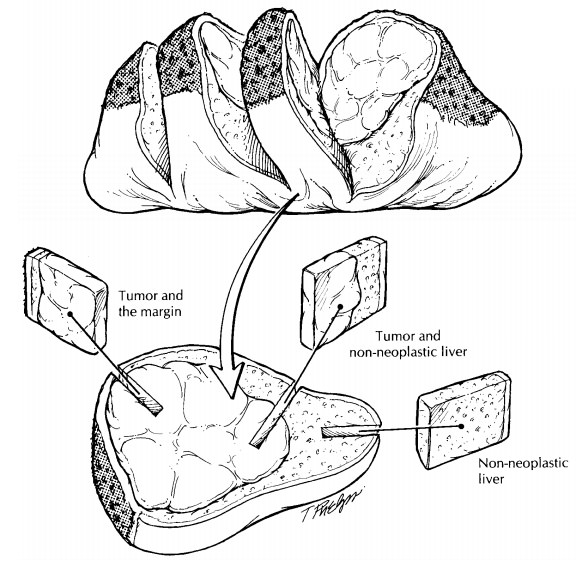
Sections
of tumors should be taken to dem-onstrate the relationship of tumor to the
sur-rounding liver parenchyma and of the tumor to the resection margin.
Sections from the periphery of the tumor are generally much more informative
than are those from the center of the tumor. The periphery of a tumor
demonstrates the interface with adjacent tissues, and the periphery of a tumor
is often less necrotic than the center. Sample the resection margin using
perpendicular sections from the areas closest to the edge of the tumor.
Depending on the extent of the resection, several representative sections of
the non-neoplastic liver parenchyma should also be submitted for histo-logic
evaluation. These sections of uninvolved liver parenchyma are generally more
informative when taken far from the nodule. In particular, sections taken
adjacent to a tumor can significantly over-estimate the degree of fibrosis.
Important Issues to Address in Your Surgical Pathology Report on Partial Hepatectomies
· What
procedure was performed, and what structures/organs are present?
· How many
tumor nodules are present? What are their sizes? Are they confined to one lobe?
· What are
the type and histologic grade of the neoplasm? Is the tumor of liver origin or
a metastasis from another site?
· Is
vascular invasion identified?
· Is the
surgical margin involved by tumor? If not, what is the distance from the margin
to the edge of the tumor?
· Does the
tumor involve lymph nodes? In-clude the number of nodes examined and the number
involved by tumor.
· What is
the condition of the non-neoplastic liver? Is the non-neoplastic liver
cirrhotic? Is there evidence of hepatitis?
Related Topics