Chapter: Medical Surgical Nursing: Oncology: Nursing Management in Cancer Care
Diagnosis of Cancer and Related Nursing Considerations
Diagnosis of Cancer and Related Nursing
Considerations
A cancer diagnosis is based on assessment for physiologic and
func-tional changes and results of the diagnostic evaluation. Patients with
suspected cancer undergo extensive testing to (1) determine the presence of
tumor and its extent, (2) identify possible spread (metastasis) of disease or
invasion of other body tissues, (3) evalu-ate the function of involved and
uninvolved body systems and organs, and (4) obtain tissue and cells for
analysis, including evaluation of tumor stage and grade. The diagnostic
evaluation is guided by information obtained through a complete history and
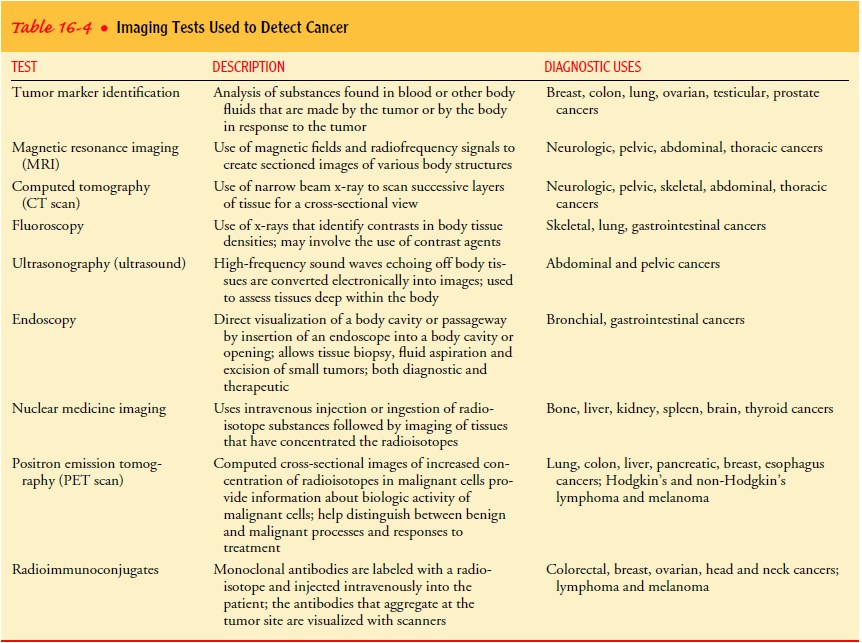
physical examination. Knowledge of suspicious symptoms and of the behavior of
particular types of cancer assists in determining which diagnostic tests are
most appropriate (Table 16-4).
A patient undergoing extensive testing is usually fearful of the procedures and anxious about the possible test results. The nurse can help relieve fear and anxiety by explaining the tests to be per-formed, the sensations likely to be experienced, and the patient’s role in the test procedures. The nurse encourages the patient and family to voice their fears about the test results, supports the pa-tient and family throughout the test period, and reinforces and clarifies information conveyed by the physician. The nurse also encourages the patient and family members to communicate and share their concerns and to discuss their questions and concerns with each other.
TUMOR STAGING AND GRADING
A complete diagnostic evaluation includes identifying the stage and
grade of the tumor. This is accomplished before treatment begins to provide
baseline data for evaluating outcomes of ther-apy and to maintain a systematic
and consistent approach to on-going diagnosis and treatment. Treatment options
and prognosis are determined on the basis of staging and grading.
Staging determines the size of the tumor and the existence ofmetastasis. Several
systems exist for classifying the anatomic ex-tent of disease. The TNM system
is frequently used. In this sys-tem, T refers to the extent of the primary
tumor, N refers to lymph node involvement, and M refers to the extent of
metasta-sis (Chart 16-3). A variety of other staging systems are used to
de-scribe the extent of cancers, such as central nervous system cancers,
hematologic cancers, and malignant melanoma, that the TNM system does not
describe appropriately. Staging systems also provide a convenient shorthand
notation that condenses lengthy descriptions into manageable terms for
comparisons of treatments and prognoses.
Grading refers to the classification of the tumor cells. Grad-ing systems seek to define the type of tissue from which the tumor originated and the degree to which the tumor cells retain the functional and histologic characteristics of the tissue of origin. Samples of cells to be used to establish the grade of a tumor may be obtained through cytology (examination of cells from tissue scrapings, body fluids, secretions, or washings), biopsy, or surgi-cal excision.
This information assists
the health care team to predict the behavior and prognosis of various tumors.
The tumor is assigned a numeric value ranging from I to IV. Grade I tumors,
also known as well-differentiated tumors, closely resemble the tissueof origin
in structure and function. Tumors that do not clearly resemble the tissue of
origin in structure or function are described as poorly differentiated or
undifferentiated and are assigned grade IV. These tumors tend to be more
aggressive and less responsive to treatment than well-differentiated tumors.
Related Topics