Chapter: Basic & Clinical Pharmacology : Histamine, Serotonin, & the Ergot Alkaloids
Basic Pharmacology of H1-Receptor Antagonists
BASIC PHARMACOLOGY OF H1-RECEPTOR
ANTAGONISTS
Chemistry & Pharmacokinetics
The
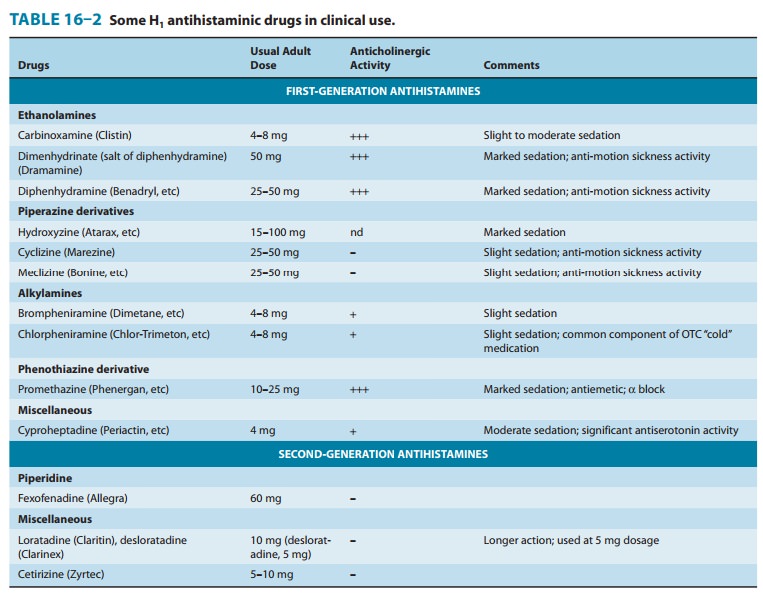
H1 antagonists are conveniently divided into first-generation and
second-generation agents. These groups are distinguished by the relatively
strong sedative effects of most of the first-generation drugs. The
first-generation agents are also more likely to block autonomic receptors.
Second-generation H1 blockers are less sedating, owing in part to
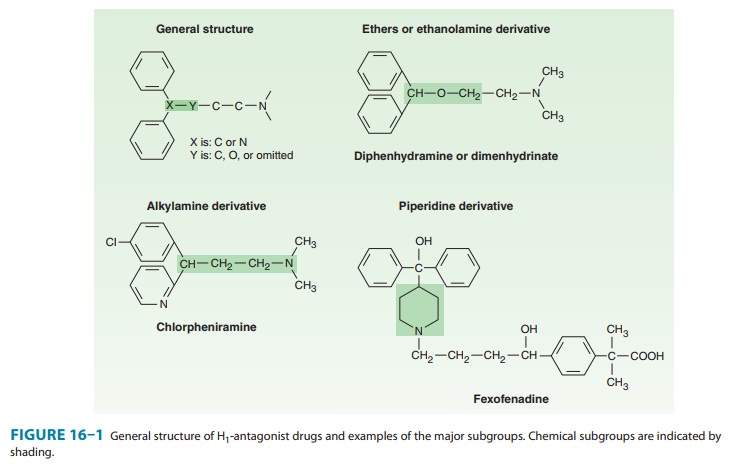
their less complete distribution into the central nervous system. All the H1
antagonists are stable amines with the general structure illustrated in Figure
16–1. Doses of some of these drugs are given in Table 16–2.
These
agents are rapidly absorbed after oral administration, with peak blood
concentrations occurring in 1–2 hours. They are widely distributed throughout
the body, and the first-generation drugs enter the central nervous system
readily. Some of them are exten-sively metabolized, primarily by microsomal
systems in the liver. Several of the second-generation agents are metabolized
by the CYP3A4 system and thus are subject to important interactions when other
drugs (such as ketoconazole) inhibit this subtype of P450 enzymes. Most of the
drugs have an effective duration of action of 4–6 hours following a single
dose, but meclizine and sev-eral second-generation agents are longer-acting,
with a duration of action of 12–24 hours. The newer agents are considerably
less lipid-soluble than the first-generation drugs and are substrates of the
P-glycoprotein transporter in the blood-brain barrier; as a result they enter
the central nervous system with difficulty or not at all. Many H1
antagonists have active metabolites. The active metabo-lites of hydroxyzine,
terfenadine, and loratadine are available as drugs (cetirizine, fexofenadine,
and desloratadine, respectively).
Pharmacodynamics
Both neutral H1 antagonists and inverse H1 agonists reduce or block the actions of histamine by reversible competitive binding to the H1 receptor.
Several have been clearly shown to be inverse
agonists, and it is possible that all act by this mechanism. They have
negligible potency at the H2 receptor and little at the H3
receptor. For example, histamine-induced contraction of bron-chiolar or
gastrointestinal smooth muscle can be completely blocked by these agents, but
the effects on gastric acid secretion and the heart are unmodified.
The
first-generation H1-receptor antagonists have many actions in
addition to blockade of the actions of histamine. The large number of these
actions probably results from the similarity of the general structure (Figure
16–1) to the structure of drugs that have effects at muscarinic cholinoceptor, α adrenoceptor,
serotonin, and local anesthetic receptor sites. Some of these actions are of
therapeutic value and some are undesirable.
1. Sedation—A common effect of first-generation H1antago-nists is sedation, but the intensity of this effect varies among chemi-cal subgroups (Table 16–2) and among patients as well. The effect is sufficiently prominent with some agents to make them useful as “sleep aids” and unsuitable for daytime use. The effect resembles that of some antimuscarinic drugs and is considered very different from the disinhibited sedation produced by sedative-hypnotic drugs. Compulsive use has not been reported. At ordinary dosages, children occasionally (and adults rarely) manifest excitation rather than sedation. At very high toxic dose levels, marked stimulation, agitation, and even convulsions may precede coma. Second-generation H1 antagonists have little or no sedative or stimulant actions. These drugs (or their active metabolites) also have far fewer autonomic effects than the first-generation antihistamines. Antinausea and antiemetic actions—Several first-generation H1 antagonists have significant activity in preventing motion sickness (Table 16–2). They are less effective against an episode of motion sickness already present. Certain H1 antagonists, notably doxylamine (in Bendectin), were used widely in the past in the treatment of nausea and vomiting of pregnancy.
2. Antiparkinsonism effects—Some of the H1antagonists,especially
diphenhydramine, have significant
acute suppressant effects on the extrapyramidal symptoms associated with
certain antipsychotic drugs. This drug is given parenterally for acute
dys-tonic reactions to antipsychotics.
3. Anticholinoceptor actions—Many first-generation
agents,especially those of the ethanolamine and ethylenediamine sub-groups,
have significant atropine-like effects on peripheral musca-rinic receptors.
This action may be responsible for some of the (uncertain) benefits reported
for nonallergic rhinorrhea but may also cause urinary retention and blurred
vision.
5. Adrenoceptor-blocking actions—Alpha-receptor
block-ing effects can be demonstrated for many H1 antagonists,
espe-cially those in the phenothiazine subgroup, eg, promethazine. This action may cause orthostatic hypotension in
susceptible indi-viduals. Beta-receptor blockade is not observed.
6. Serotonin-blocking action—Strong blocking effects at sero-tonin receptors have been demonstrated for some first-generation H1 antagonists, notably cyproheptadine. This drug is promoted as an antiserotonin agent and is discussed with that drug group. Nevertheless, its structure resembles that of the phenothiazine antihistamines, and it is a potent H1-blocking agent.
7. Local anesthesia—Several
first-generation H1antagonistsare potent local anesthetics. They
block sodium channels in excit-able membranes in the same fashion as procaine
and lidocaine. Diphenhydramine and promethazine are actually more potent than
procaine as local anesthetics. They are occasionally used to produce local
anesthesia in patients allergic to conventional local anesthetic drugs. A small
number of these agents also block potas-sium channels; this action is discussed
below (see Toxicity).
8. Other actions—Certain H1antagonists,
eg, cetirizine, inhibitmast cell release of histamine and some other mediators
of inflam-mation. This action is not due to H1-receptor blockade and
may reflect an H4-receptor effect . The mechanism is not fully
understood but could play a role in the beneficial effects of these drugs in
the treatment of allergies such as rhinitis. A fewH 1 antagonists
(eg, terfenadine, acrivastine) have been shown to inhibit the P-glycoprotein
transporter found in cancer cells, the epithelium of the gut, and the
capillaries of the brain. The signifi-cance of this effect is not known.
Related Topics