Chapter: Ophthalmology: Optic Nerve
Atrophy of the Optic Nerve
Disorders in which the Margin of the Optic Disk is Well Defined
Atrophy of the Optic Nerve
Definition
Irreversible loss of axons in the region of
the third neuron (from the retinal layer of ganglion cells to the lateral
geniculate body).
Morphology and pathologic classification:
Atrophy of the optic nerve isclassified
according to its morphology and pathogenesis. The following forms are
distinguished on the basis of
ophthalmoscopic findings:
❖ Primary atrophy of the optic nerve.
❖ Secondary atrophy of the optic nerve.
❖ Glaucomatous atrophy of the optic nerve.
Forms of primary atrophy of the optic nerve
may be further classified accord-ing to their pathogenesis:
❖ Ascending atrophy in which the lesion is located anterior to the lamina
cri-brosa in the ocular portion of the optic nerve or retina.
❖ Descending atrophy in which the lesion is located posterior to the
laminacribrosa in a retrobulbar or cranial location.
Etiology:
Etiology of primary atrophy of the optic nerve.
The most important causes are as follows:
❖ Ascending atrophy (after two to four weeks):
– Usually vascular, such as central retinal
artery occlusion or anterior ischemic optic neuropathy.
❖ Descending atrophy
(after four to six weeks):
– Compressive, such as from an orbital or
intracranial mass or hydro-cephalus.
– Traumatic, such as avulsion, compression of
the optic nerve in a frac-ture, or hematoma in the optic nerve sheath.
– Inflammatory, such as retrobulbar optic
neuritis, arachnoiditis of the optic chiasm, or syphilis.
❖ Toxic:
– Chronic abuse of low-grade tobacco and
alcohol in tobacco and alcohol amblyopia.
– Lead,
arsenic, or thallium.
–
Methyl alcohol.
– Medications, such as ethambutol,
chloramphenicol, gentamicin, isoni-azid, vincristine, penicillamine, etc.
❖ Congenital or hereditary:
– Infantile hereditary optic atrophy (an
autosomal dominant disorder with slow progressive loss of visual acuity, color
vision defects, and visual field defects.
– Juvenile hereditary optic atrophy (similar
to the infantile form only the onset is usually later, in the second decade of
life).
–
Leber’s optic atrophy.
–
Behr’s infantile recessive optic atrophy.
❖ Systemic disorders:
–
Hemorrhagic anemia or pernicious anemia.
–
Leukosis.
Etiology of secondary atrophy of the optic nerve.
The most important causes are as follows:
❖ Papilledema.
❖Anterior ischemic optic neuropathy.
❖ Papillitis.
The etiology of any atrophy of the optic nerve
should be determined to exclude possible life-threatening intracerebral causes
such as a tumor.
Symptoms:
The spectrum of functional defects in optic atrophy is
broad.These range from small peripheral visual field defects in partial optic
atrophy to severe concentric visual field defects or blindness in total optic
atrophy.
Diagnostic considerations:
The most important examinations are a detailedhistory,
ophthalmoscopy, and perimetry testing. Color vision testing and visual evoked
potential may be useful as follow-up examinations in begin-ning optic atrophy.
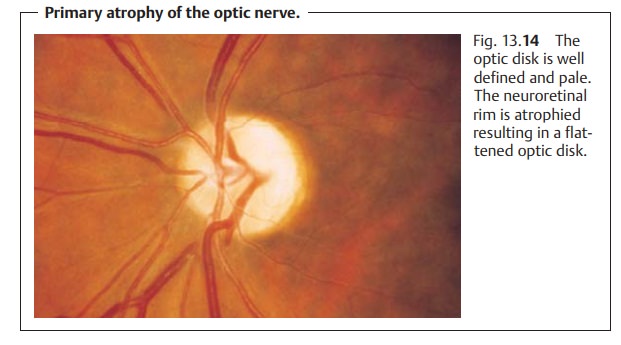
Primary atrophy of the optic nerve.Ophthalmoscopy will reveal a welldefined, pale optic disk (Fig.
13.14). The pallor can cover the
entire optic disk (it will appear chalk white in total optic atrophy), or it
may be partial or seg-mental. The neuroretinal rim is atrophied, which causes
the optic disk to flat-ten out. The diameter of the retinal vessels will be
decreased.
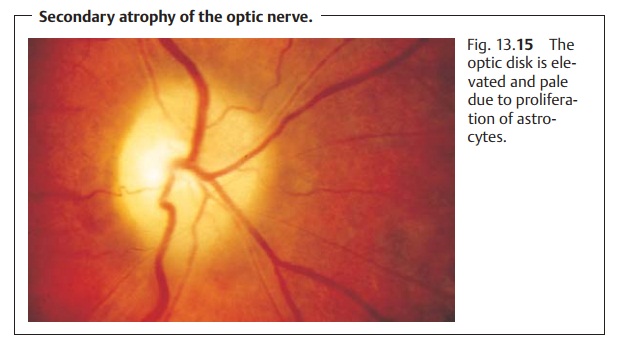
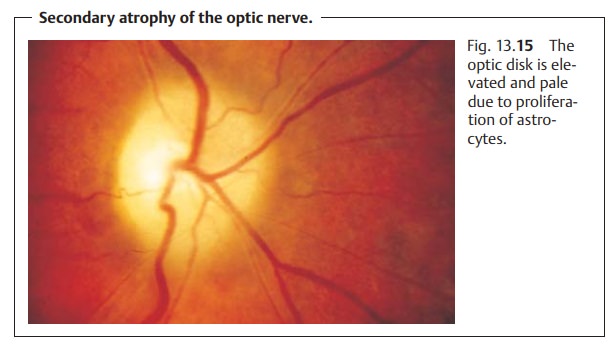
Secondary atrophy of the optic nerve.Ophthalmoscopy will reveal a paleoptic disk.
The disk is slightly elevated due to proliferation of astrocytes, and the
margin is blurred (Fig. 13.15). The
optic cup will be partially or completely obscured. The retinal vessels will be
constricted.
Treatment:
The disorder involvesirreversibledamage
to the nerve fibers. As aresult, no effective treatment is available.
Prognosis:
Early identification and timely management of a treatable causesuch as a tumor or pernicious anemia can arrest the progression of the dis-order. Where this is not the case, the prognosis for vision is poor.
Special Forms of Atrophy of the Optic Nerve
Leber’s atrophy.Here there is involvement of both optic nerveswithout addi-tional neurologic symptoms.
In 85% of all cases, men between the ages of 20and 30 are affected. The
disorder is due to mutations in the mitochondrial DNA.
Ophthalmoscopy will reveal optic disk edema as in papillitis followed byprimary
optic nerve atrophy. Initial retrobulbar optic neuritis is also possible.
Functional symptoms include a large central scotoma with a peripherallylimited
visual field. This will lead to significant loss of vision within a few months,
although the remaining vision will not decrease any further.
There is no treatment.
Behr’s disease (infantile recessive optic atrophy).This is also a disorderinvolving both optic
nerves. However, in contrast to Leber’s atrophy there are additional neurologic symptoms. These may include ataxia and mental
retar-dation. The disease is an inherited autosomal recessive disorder and
manifests itself in early childhood.
Ophthalmoscopy will reveal progressive optic atrophy with severe loss ofvisual
acuity but without complete blindness.
There is no treatment.
Waxy pallor optic atrophy.This disorder (Fig. 13.16) is associated with tape-toretinal
degeneration, such as retinitis pigmentosa.
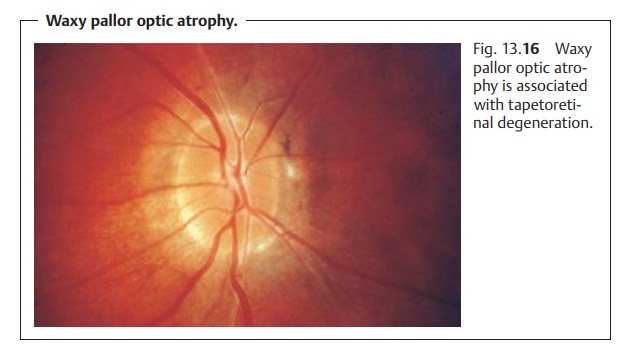
Ophthalmoscopy will reveal an optic disk
with a wax-like pallor that is shal-low with a well defined margin. There
will be severe thinning of the central retinal vessels. The cause of the wax-like yellow color is not
known.
There is no treatment.
Related Topics