Chapter: Obstetric and Gynecological Nursing : Normal Pregnancy
The Third Stage of Labour
3. The Third Stage of Labour
It begins immediately after the baby is born, until the placenta is
delivered. The third stage lasts between 5-15 minutes but any period upto 1
hour is normal. If it lasts more than 1 hr it is considered as retained
placenta.
Physiology of the third stage of labour
·
Separation of the placenta
·
Descent of the placenta
·
Expulsion of the placenta
·
Control of bleeding
1. Separation of the placenta
Mechanism of placental
separation
It is brought by the contraction and retraction of the uterine musules.
Separation usually begins in the center of the placenta. At the area of the
separation the blood sinuses are torn across. 30to 60ml of blood is connected
between maternal surface of the placenta and the decidual basalis. The uterine
contractions detaches the placenta from the uterus and the placenta forced out
of the upper uterine segment into the lower utrine segment.
1. Centeral separation
Advantage – Centerally retro placental clot is formed
Aids separation by exerting pressure at the mid point of placental
attachment and helps to strip the adherent lateral boarders to peel the
memberanes off the uterine wall
2. Separation begins at the level of the deep
sponge layer of the deciduas. If the placenta is embedded deeply separation
will be difficult.
3. Separation occurs at the lower edge of
placenta
Signs for placental separation
·
Gush of blood
·
The fundus rises at the level of umblicus
·
Uterus becomes globular
·
Cord lengthen
The uterus contracts during & after the birth of the baby. This
causes the uterus to become smaller, the placenta remains the same size &
is pushed off the uterine wall.
2. Descent of the placenta
When the placenta has completely separated, the constructing uterus
pushes it down into the lower uterine segment and into the vagina. The weight
of the placenta itself pulls the chorine of the uterine wall.
Sign of placental descent
·
The uterus becomes hard, round and movable.
·
The fundus rises to the level of the umbilicus.
·
The cord seems to lengthen.
·
There is a gush of blood
·
When you apply suprapubic pressure the cord will not received back
·
Placenta can be feet on vaginal examination.
3. Expulsion of the placenta
Method of placental expulsion
·
Using the fundus as a piston
The contracted fundus is used as apposition to push the placenta out.
·
Controlled cord traction with oxytocin drugs
·
Controlled cord traction with out oxytoin drugs (Brandit Andreivs
method)
·
Fundal pressure
·
Traditional method/Bearing down by the woman/
1. Controlled cord traction with
oxytocic drugs /Active management of third stage of labour/
Definition -Adminstration of oxytocic drugs with birth of the anterior shoulder and application of controlled cord traction
with first uterine contraction.
Advantages:
·
Shorten the third stages
·
Reduce blood loss and the incidence of hemorrhage in risk cases
Methods
·
An oxytocic drug is given /if pregnancy is not multiple/ as soon as
anterior shoulder is delivered.
·
The cord is clamped and cut, wait for contraction.
·
Donot wait for the sign of placental separation and descent
·
As soon as the uterus contracts the left hand is placed above the
symphysis pubis push and the uterus upwards to words the umbilicus. At the same
time the right hand grasps the umbilical cord and apply traction in “a down
ward direction” out ward when the placenta is visible traction is exerted in an
upward direction following the curves of then birth canal and then deliver the
placenta.
If the membranes are not complete twisting the placenta to form the membranes
in to a rope or grasping the membranes with artery forceps and move gently up
and down to remove it. It is done for high risk mothers.
Recommendations – When active management of the
thirdstage is used clamp the cord.
2. Controlled cord traction with out oxytocic drugs /Brandit Andrews method/ passive management of third stage of labour
Signs of placental separation and descent are awaited. The left hand is
placed above the symphysis pubis push the uterus upwards towards the umbilicus.
At the same time the right hand grasps the umbilical cord and apply traction in
“a down ward direction” out ward when the placenta is visible traction is
exerted in an upward direction following the curves of the birth canal then
deliver the placenta.
Cord traction should not be applied when the fetus is macerated or if
the baby is preterm.
Danger: Breaking of the cord. If the cord is snap manual removal is
indicated.
Advantage: It allows the placenta to separate and descend with out
interference
Danger: The third stage may be longer
Haemorrhage and infection may happen
3. Maternal effort: When the uterus is well
contracted ask themother to push as she did during the birth of the baby. If
she is not successful, the midwife or nurse may put a hand flat on the abdomen
while the mother pushes, thus provides counter pressure to compensate the poor
abdominal muscle tone.
4. Fundal pressure: The midwife or nurse puts her
left handon the fundus of the well contracted uterus and pushes down wards and
back wards. The uterus is pushed against the placenta and the placenta emerges
from the vagina, receive the placenta, massage the uterus to make it contract,
and give Ergometrine.
Indication:- Preterm labour, still birth
Danger- Pain
N.B Fundal pressure and cord
traction must never becombined because of the risk of inversion of the uterus.
5. Traditional method
Up right kneeling/ squatting positions should be recommended when the
third stage is passively managed. Gravity and intra abdominal pressure aid
& speed the process Advantage – Blood loss can be easily observed
About 500-.800ml blood flows through the placental site each minute.
Following delivery of the placenta the oblique muscle fibers of the myometrium
contract very strongly to compress the blood vessels.
All average blood loss after the delivery of the placenta is 150ml.
Blood loss should never be more than 500ml. All blood should be measured
including clots from the placental surface.
Examination of the placenta, membrane and umbilical cord
Inspect the fetal side:-
·
Check the location of the insertion of the cord /central, marginal or
velamentous
·
Trace blood vessels on the periphery to detect any torn vessels. It
indicates a succentarete or extra lobe of the placenta.
· Check second hole on the memberane
Inspect the umbilical cord
·
Check the number of blood vessels /two artery and one vein/
·
Check the length of the cord.( Long-50-55cm or short)
· Check for the presence of a true knot or abnormalities
Inspect the maternal side:
·
Check the cotyledons
·
Observe for areas of Abruption, infarction or calcification
4. Control of bleeding
Methods:-
- Contraction & relaxation of uterine muscles
- The actions of living ligatures
-Extra clothing power in the blood
The third stage is the shortest and easiest but the most dangerous
stage. Bleeding after third stage of labour stops spontaneously, because of:
·
“Living ligatures” The oblique muscles fibers of the uterus run in and
out between the blood vessels when the uterus is contracted they clump the
blood vessels very securely and the bleeding stops.
·
Extra clotting power: The mother has extra clothing power in her blood
at this time the clotting mechanism is very powerful.
At the end of the third stage
·
The uterus should be hard, round and movable
·
The uterus should be mid way between the umbilicus and sympysis puleis
·
There should be no bleeding
·
The bladder should be empty
The Oxytocic Drugs
These drugs stimulate the uterus to contract. It is used before, during
& after the third stage of labour.
Advantages:
·
It speeds up the delivery of the placenta
·
Lessen the blood loss
·
Contract the uterus
The oxytocin drugs are:-
· Syntocinan, orastinon, pitocin,
oxytocin one ampule contains 5 or 10 units
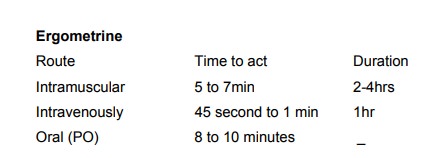
· Ergometrine ampules – 0.5 mg or
0.25mg Ergometrine 0.25 or 0.5mg tablet form
· Syntometrine1ml contains 0.5mg
Ergometrine and 5 unites of oxytocin.
· Ergometrine:- It is given during
or after the third stage of labour
Indications
·
To prevent or treat PPH
·
To prevent bleeding in inevitable complete or incomplete abortion
·
To treat sub involution during the puerperium
Contraindications: - It should not given for pre-eclamptic, cardiac and
hypertensive mothers
Pitocin /oxytocin synotcinon, orastinon
Actions: - To contract the smooth muscle
Advantages – It can be given before or at any stage of labour (1st, 2nd or 3rd of labour) It has a rapid
action
Indication:
·
To induce /start/ labour
·
To accelerate /increase/ the contractions in labour
·
To prevent or treat post partum haemorrhage
Caution – The uterine contractions and fetal heart are continuously
monitored
Contraindications- In the presence of malpresentation or C.P.D it is not
start.
Danger
·
Rupture of the uterus
·
Tachycardia & an increased stroke volume increases the cardiac out
put.
·
Fetal distress
Syntometrine
It is a combined preparation of Ergometrine and oxytocin
Action:
1 ampule of syntometrine contains
·
Egometrine 0.5mg
·
Syntocinon 5 units
Action 2 ½ minutes when given intramuscular
Advantage- It has the quick action of the oxytocin and the long action
of ergometrine
Indication - to prevent or treat post partum haemorrhage
Management of third stage of labour
Good management begins during prenatal period. In the 1st, 2nd and 3rd stage of labour to prevent
prolonged labour Skill full management reduces the risk of hemorrhage, retained
placenta, shock and infection
The guiding principles is to watch and wait and not to interfere Rubbing
the fundus causes irregular uterine activity which partly separate the placenta
and allows bleeding
Position of the mother – the dorsal position
Advantages
·
more comfortable to the mother
·
cord traction is applied more effectively
·
injuries to the birth canal is observed
Bleeding before placental delivery is due to:-
·
Partial separation of the placenta
·
Uterine relaxation
Prolonged third stage is due to:-
·
Weak uterine contraction which causes failure of the placenta to
separate
·
Adherent placenta
· Full bladder
Danger: - Post partum hemorrhage and shock
If the fundus is more than 2.5cm above the umbilicus four cases must be
considered.
a.
There is another baby in uterus
Palpate for fetal parts, auscultate for a fetal heart beat
b.
The placenta is unduly large
causes- Rh negative baby suffered from hydrops
fetalis
c.
Blood clot is present in the uterus
This will prevent strong contraction of the uterus and cause post partum
haemorrhage (contraction of oblique muscles of myometrium)
d. Full bladder
Clamping and cutting of the umbilical cord
The choices:
A. Clamp the cord soon after birth /1-3 minutes/ before it stops
pulsation or
B. Wait until cord has stopped pulsating before clamping leave the
maternal end of the cord unclamped when cord is cut.
A. Early cord clamping
Advantages: The length of the third stage of labour is reduced
Disadvantages: preterm babies have an increased incidence of respiratory
distress.
Early cord clamp is associated with lower haematocrit and levels in the
baby. It increases the risk of Feto – maternal transfusion – Rhesus negative
mothers caring rhesus positive babies are more likely to develop Antibodies
B. Delayed cord clamping
The cord clamp should be delayed for preterm babies and rhesus negative
mothers
Advantages- Preterm babies will benefit from resulting increase in circulating blood, and higher neonatal haematocrit and hemoglobin should be obtained Disadvantages – over loading the baby’s system
C. Leaving maternal end of the cord unclamped when cord is cut
Before allowing the maternal end of the cord to remain unclamped, a
second twin must be excluded.
Advantages
There is less blood loss
·
Lower incidence of manual removal of the placenta
·
Rhesus negative mothers carrying rhesus positive babies are less likely
to develop antibodies
Disadvantages – A second twin may die when it is unclamp
Related Topics