Chapter: Obstetric and Gynecological Nursing : Normal Pregnancy
The Fetal Circulation
The Fetal Circulation
At the birth there is a dramatic alteration in this situation and almost
instaneous change must occur. Besides this all, the postnatal structures must
be in place and ready to take over. There are several temporary structures
inaddition to the placenta itself and the umblical cord and these enable the
fetal circulation to take place while allowing for the changes at birth.
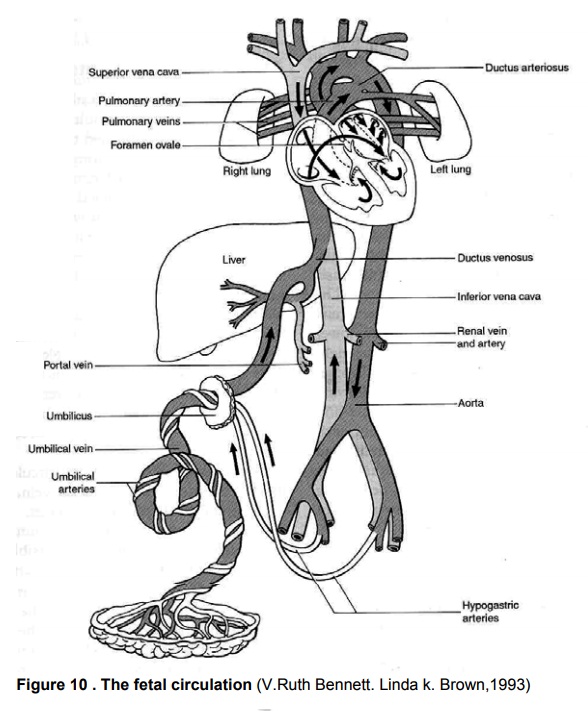
The Umbilical vein Leads from the umblical cord to
theunderside of the liver and carries blood rich in oxygen and nutrients. It
has a branch which joins the portal vein and supplies the liver.
The ductus vensous (from a vein to a vein) connects
theumblica vein to the inferior venacava. At this point the blood mixes with
deoxygenated blood returning from the lower parts of the body. Thus the blood
throughout the body is at best partially oxygenated.
The foramen ovale (oval opening) is a temporary
openingbetween the atria which allows the majority of blood entering from the
inferior vencava to pass across into the left atrium. The reason for this
diversion is that the blood does not need to pass through the lungs since it is
already oxygenated.
The ductus arteriosus (from an artery to an artery)
leadsfrom the bifuraction of the pulmonary artery to the descending aorta,
entering it just beyond the point where the subclavian and carotid arteries
leave.
The hypogastric arteries branch off from the internal
iliacarteries and become umbilical arteries when they enter the umblical cord.
They return blood to the placenta. This is the only vessel inthe fetus which
carries unmixed blood.
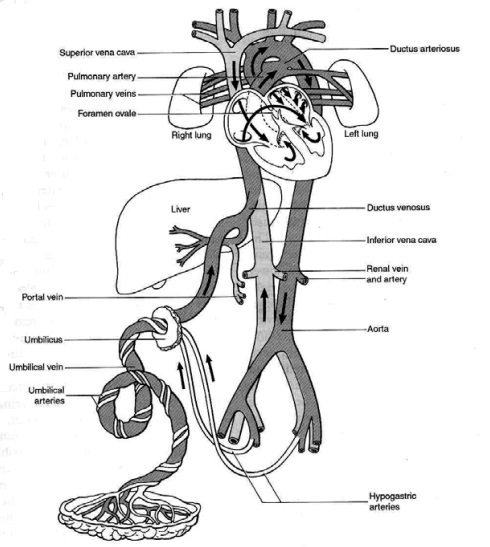
Figure. The fetal circulation
Adaptation to extra Uterine life
At birth the baby takes a breath and blood is drawn to the lungs through
the pulmonary arteries. It is then collected and returned to the left atrium
via the pulmonary veins resulting in a sudden inflow of blood. The placental
circulation ceases soon after birth and so less blood returns to the right side
of the heart. In this way the pressure in the left side of the heart is greater
while that in the right side of the heart becomes less. This results in the
closure of a flop over the formaen ovale which separated the two sides of the
heart and stops the blood flowing from right to left.
The cessation of the placenta circulation results in the collapse of the
umbilical vein, the ductus venosus and the hypogastric arteries. These vesels
after collapse change to the following structure.
The umbilical vein → the ligamentaum teres
The ductus venosus → the ligamentum venosum
The ductus arteriosus → the ligamentum arteriousm
The foramen ovale → the Fossa ovalis
The hypogastric arteries → the obliterated hypogastic arteries
The Placental Circulation
The placenta is completley formed and functioning from 10weeks after
fertilization. Between 12 and 20 weeks gestation the placenta weighs more than
the fetus.Fetal blood, low in oxygen, is pumped by the fetal heart towards the
placenta along the umblical arteries. Having absorbed oxygen the blood is
returned to the fetus via the umblical vein.
Appearance of the Placenta at Term
The placenta measures about 20 cm in diameter and 2.5cm thick from its
center. It weighs approximately one sixth of the baby’s weight at term. It has
two surfaces.
i.
The maternal surface maternal blood gives this surface a dark red colour
and part of the basal decidua will have beenseparated with it. The surface is
arranged in about 20 lobes which are separated by sulci
ii.
The fetal surface. The amnion covering the fetal surface of the placenta
gives it a whitish, shiny appearance. Branches of the umbilical veins and
arteries are visible and spreading out from the insertion of the umbilical cord
which is normally in the center.
The aminotic sac consists of a double memberane.
Chorion – Outer layer adher to the
uterine wall.
Amnion.-The inner layer of the
aminotic sac containing anaminotic fluid and cover the fetal surface of the
placenta and are what give the placenta its typical shiny appearance.
Protects the fetus from any infection and the amniontic fluid is a
clear, pale straw in colour.It secreted by the amnion and fetal urine also
contributes to the volume from the 10th weeks of the gestation on wards.The total
amount of amniotic fluid is about 1 litter and diminished to 800ml at 38 weeks
of gestation (term). If the total amount exceeds 1500 ml, the condition is
known as polyhdramnous and if less than 300ml it is known as oligohydraminous.
It constitutes 99% water and the remaining 1% is dissolved organic maters
including substances and waste products.
Function
i.
Allows for free movement of the fetus
ii.
Protects the fetus from injury
iii.
Maintains aconstant temperature for the fetus
iv.
During labour it protects the placenta and umblical cord from the
pressure of uterine contraction
v.
Aids effeciement of the cervix and dilation of the uterineos
Related Topics