Chapter: Medicine and surgery: Endocrine system
Syndrome of inappropriate anti diuretic hormone secretion (SIADH) - Thirst axis
Thirst axis
Syndrome of inappropriate anti-diuretic hormone secretion (SIADH)
Definition
SIADH is characterised by the persistence of ADH secretion despite decreased plasma osmolality and normal or increased extracellular fluid volume.
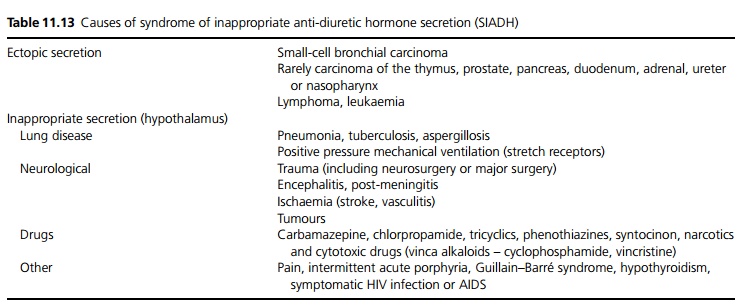
Aetiology
See Table 11.13.
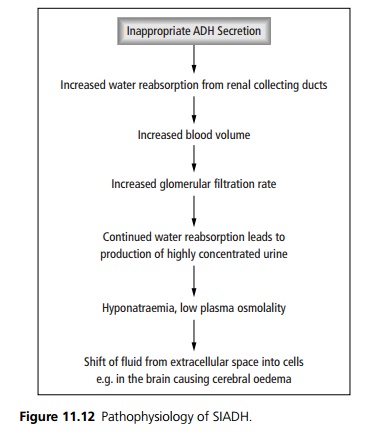
Pathophysiology
ADH is a peptide hormone similar to oxytocin which is normally secreted from the posterior pituitary, in response to an increase in plasma osmolality. It acts on the collecting tubules in the kidney to make them more permeable to water molecules. Hence its secretion causes water retention (see Fig. 11.12).
Clinical features
Patients present with headache, confusion, behavioural changes, convulsions and coma. On examination there is no peripheral oedema. There may be muscle twitching with an extensor plantar reflex.
Investigations
Electrolyte analysis will reveal hyponatraemia with reduced plasma osmolality, and high urinary osmolality and sodium. Plasma osmolality can be estimated from the sodium, urea and glucose concentrations (Ôł╝2x [Na] + [Urea] + [glucose]).
Management
Fluid restriction is the mainstay of treatment, although this is unpleasant for the patient and often difficult to enforce. It is also a useful diagnostic test. Demeclocycline, an ADH antagonist at the renal collecting ducts can be used, but is nephrotoxic, especially in the elderly. If water intoxication is severe, diuretics with hypertonic saline infusion is used. Any underlying cause should be identified and treated.
Prognosis
In many cases the syndrome is temporary.
Related Topics