Chapter: Medicine and surgery: Endocrine system
Diabetes insipidus - Thirst axis
Diabetes insipidus
Definition
Polyuria, thirst & polydipsia resulting from deficiency of or resistance to antidiuretic hormone (vasopressin).
Aetiology
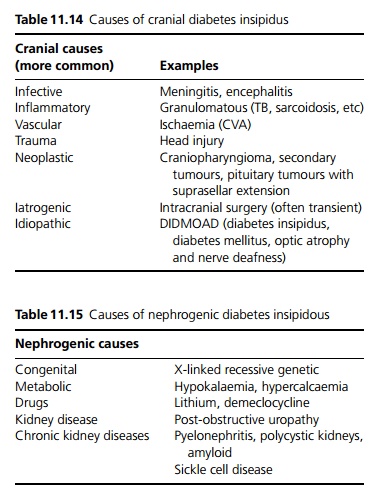
Diabetes insipidus results from either a deficiency in anti diuretic hormone (central or cranial diabetes insipidus, see Table 11.14) or from renal resistance to ADH (nephrogenic diabetes insipidus, see Table 11.15).
Pathophysiology
Normally ADH acts on the renal collecting ducts to increase water reabsorption preventing plasma osmolality from rising. Lack of vasopressin, or renal resistance to vasopressin leads to loss of water (water depletion), leading to polyuria. Unless the thirst centre is also impaired, rising osmolality stimulates thirst and the person drinks water in increased quantities. The urine is dilute.
Clinical features
Polyuria, polydipsia. Daily urine output may be >10 L a day.
Complications
Hypernatraemia if patient is denied access to water or is unconscious. If left untreated there is progression to severe irreversible brain damage and cerebral vessels may tear causing intracranial haemorrhage. Rapid rehydration can cause a similar problem.
Investigations
Plasma osmolality is normal to high (>295 mmol/kg) with associated hypernatraemia, The urine osmolality is low. In the water deprivation test the patient is weighed, plasma and urine osmolality measured, then they are deprived of fluid for 8 hours under constant supervision.
┬Ě Diabetes insipidus is diagnosed if body weight falls by >3%, if plasma osmolality exceeds 300 mmol/kg, or if the urine:plasma osmolality ratio remains <1.9 (provided plasma osmolality exceeds 285 mmol/kg).
┬Ě After 8 hours, the patient is allowed to drink freely and desmopressin (DDAVP ÔÇô desamino-D-arginine vasopressin, a long-acting vasopressin analogue) is given intranasally or i.v. Urine output is monitored.
┬Ě If the kidneys are then able to produce concentrated urine the diabetes insipidus is due to ADH deficiency, i.e. central diabetes insipidus. If the urine remains dilute the kidneys are insensitive to ADH, i.e. nephrogenic diabetes insipidus.
Management
Any underlying cause should be sought and treated if possible. DDAVP intranasally is used in cranial diabetes insipidus. There is no specific treatment for nephrogenic diabetes insipidus.
Related Topics