Chapter: Medicine and surgery: Endocrine system
Growth axis
Growth axis
Growth hormone releasing hormone (GHRH or GRH) secreted from the hypothalamus in a pulsatile manner. Growth hormone (GH also called somatotrophin) promotes linear growth mainly through insulin-like growth factor (IGF-I previously known as somatomedin C), see Fig. 11.5.
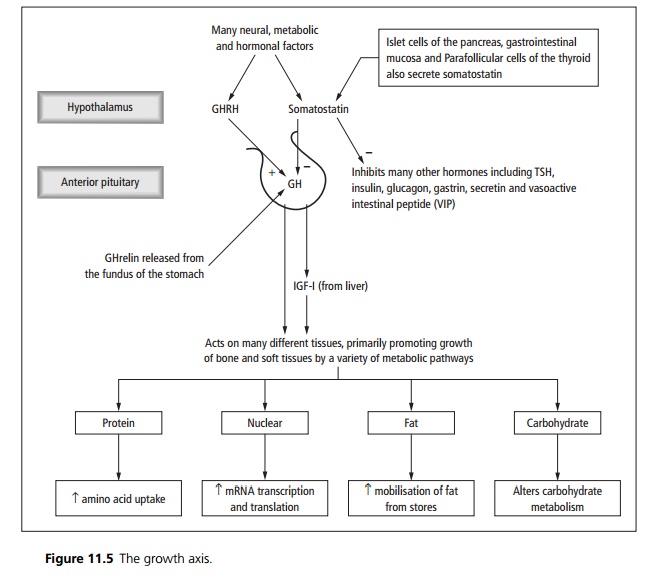
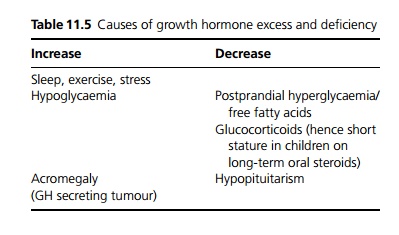
Conditions that affect levels of growth hormone are shown in Table 11.5.
Acromegaly
Definition
Acromegaly is a clinical syndrome caused by growth hormone (GH)-secreting pituitary adenomas in adults.
Incidence
GH-secreting pituitary adenomas are second in fre-quency to prolactinomas.
Age
Can occur at any age but mean onset 40 years.
Sex
M = F
Aetiology
95% of cases result from growth-hormone-secreting
pituitary adenoma (somatotroph). A mutation in the Gs protein leading to excessive cAMP production has been found in 40% of GH-secreting adenomas. Acromegaly may occur as part of multiple endocrine neoplasia (MEN) type I.
In around 5% of cases there is ectopic GHRH secretion from a carcinoid tumour, GH from a pancreatic islet cell tumour, or inappropriate hypothalamic production of GRH.
Pathophysiology
Excess production of GH leads to the release of high levels of IGF-I (insulin-like growth factor) from the liver.
The combination of high levels of GH and IGF-I leads to following:
┬Ě Overgrowth of bone and soft tissue, particularly the face and skull.
┬Ě These hormones are lipolytic, diabetogenic and cause sodium and water retention. Other endocrine and metabolic abnormalities may occur, due to the local mechanical effect of the adenoma on normal pituitary tissue.
Clinical features
The course of the disease is slowly progressive. Soft tissue overgrowth is the characteristic early feature, causing enlargement of hands and feet, coarse facial features.
Face and skull: Thickened calvarium, prominent supraorbital ridges, enlarged nose, prognathic mandible, widely spaced teeth and puffiness of the face due to soft tissue overgrowth.
Hands and feet are bulky, with blunt, spade-like fin-gers.
Bones and joints: Arthralgia and degenerative arthritis of the spine, hips and knees due to bone and cartilage overgrowth. Carpal tunnel syndrome is common.
Skin is thickened, oily and sweaty. Acne, sebaceous cysts and skin tags are common. Acanthosis nigricans of the axillae and neck may occur. Hypertrichosis in women.
Cardiovascular: Hypertension in 25% of patients, and left ventricular hypertrophy and cardiomyopathy leading to cardiac failure in about 15%.
Organomegaly: Thyroid and salivary gland enlargement, hepatomegaly.
Diabetes in 40% of patients.
Macroscopy/microscopy
The tumour is solid and trabecular, often 1 cm in diameter by the time of diagnosis. Immunohistochemistry can be used to stain for GH.
Complications
Renal calculi occur in 10% as a result of the hypercalciuria induced by GH excess.
Local effects of a pituitary tumour include headache, and pressure effects such as bitemporal hemianopia. Panhypopituitarism may occur.
Increased risk of uterine tumours and possibly of colonic polyps.
Investigations
IGF-I and GH levels are raised, but GH levels are unreliable due to episodic secretion. An oral glucose suppression test is performed ÔÇô a glucose load will fail to suppress growth hormone production.
Imaging of the pituitary fossa by X-ray, CT or MRI. If there is no evidence of a pituitary adenoma GHRH
may be assayed.
Management
Wherever possible transphenoidal resection of the adenoma is the treatment of choice. Large tumours may be resected by transfrontal craniotomy. Prior to surgery hypopituitarism must be treated using cortisol and thyroxine.
Octreotide or lanreotide, a long-acting somatostatin analogue, may be used prior to surgery, following in-complete resection or in elderly patients not fit for surgery. Dopamine agonists may be added in refractory cases.
Irradiation may be used as an adjuvant to other therapies.
Accompanying hypopituitarism is treated as appropriate with corticosteroids, thyroxine and gonadal steroids or gonadotrophins.
Prognosis
Follow-up is required for recurrence or loss of pituitary function. Acromegaly causes increased morbidity and mortality mainly due to diabetes and cardiovascular disease.
Related Topics