Chapter: Medical Surgical Nursing: Management of Patients With Neurologic Dysfunction
Seizure Disorders
Seizure Disorders
SEIZURES
Seizures are episodes of abnormal motor, sensory,
autonomic, or psychic activity (or a combination of these) resulting from
sud-den excessive discharge from cerebral neurons (Greenberg, 2001; Hickey,
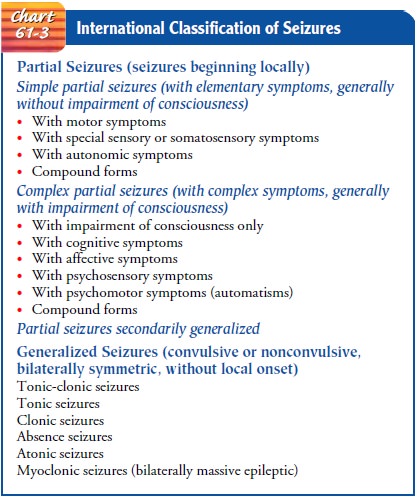
2003). A part or all of the brain may be involved. The international
classification of seizures differentiates between two main types: partial
seizures that begin in one part of the brain, and generalized seizures that
involve electrical discharges in the whole brain (Chart 61-3). Most seizures
are sudden and transient.
The underlying cause is an electrical disturbance
(dysrhyth-mia) in the nerve cells in one section of the brain, causing them to
emit abnormal, recurring, uncontrolled electrical discharges. The
characteristic seizure is a manifestation of this excessive neu-ronal
discharge. There may be associated loss of consciousness, excess movement or
loss of muscle tone or movement, and dis-turbances of behavior, mood,
sensation, and perception.
The specific causes of seizures are varied and can
be catego-rized as idiopathic (genetic, developmental defects) and acquired.
Among the causes of acquired seizures are hypoxemia of any cause, including
vascular insufficiency, fever (childhood), head injury, hypertension, central
nervous system infections, metabolic and toxic conditions (eg, renal failure,
hyponatremia, hypocal-cemia, hypoglycemia, pesticides), brain tumor, drug and
alcohol withdrawal, and allergies (Schumacher, Pruitt & Phillips, 2000).
Cerebrovascular disease is the leading cause of seizures in the elderly
(Berges, Moulin, Berger et al., 2000).
Nursing Management During a Seizure
A major responsibility of the nurse is to observe
and record the sequence of symptoms. The nature of the seizure usually
indicates the type of treatment that is required (Wulf, 2000). Before and
during a seizure, the following are assessed and documented:
·
The circumstances before the
seizure (visual, auditory, or olfactory stimuli, tactile stimuli, emotional or
psychologi-cal disturbances, sleep, hyperventilation)
·
The occurrence of an aura
(visual, auditory, or olfactory)
·
The first thing the patient
does in a seizure—where the movements or the stiffness starts, conjugate gaze
position, and the position of the head at the beginning of the seizure. This
information gives clues to the location of the seizure origin in the brain. (In
recording, it is important to state whether the beginning of the seizure was
observed.)The type of movements in the part of the body involved
·
The areas of the body involved
(turn back bedding to ex-pose patient)
·
The size of both pupils. Are
the eyes open? Did the eyes or head turn to one side?
·
The presence or absence of
automatisms (involuntary motor activity, such as lip smacking or repeated
swallowing)
·
Incontinence of urine or stool
·
Duration of each phase of the
seizure
·
Unconsciousness, if present,
and its duration
·
Any obvious paralysis or
weakness of arms or legs after the seizure
·
Inability to speak after the
seizure
·
Movements at the end of the
seizure
·
Whether or not the patient
sleeps afterward
·
Cognitive status (confused or
not confused) after the seizure
In
addition to providing data about the seizure, nursing care is directed at
preventing injury and supporting the patient. This includes supporting the
patient not only physically but also psy-chologically. Consequences such as
distress, embarrassment, fa-tigue, and depression can be devastating to the
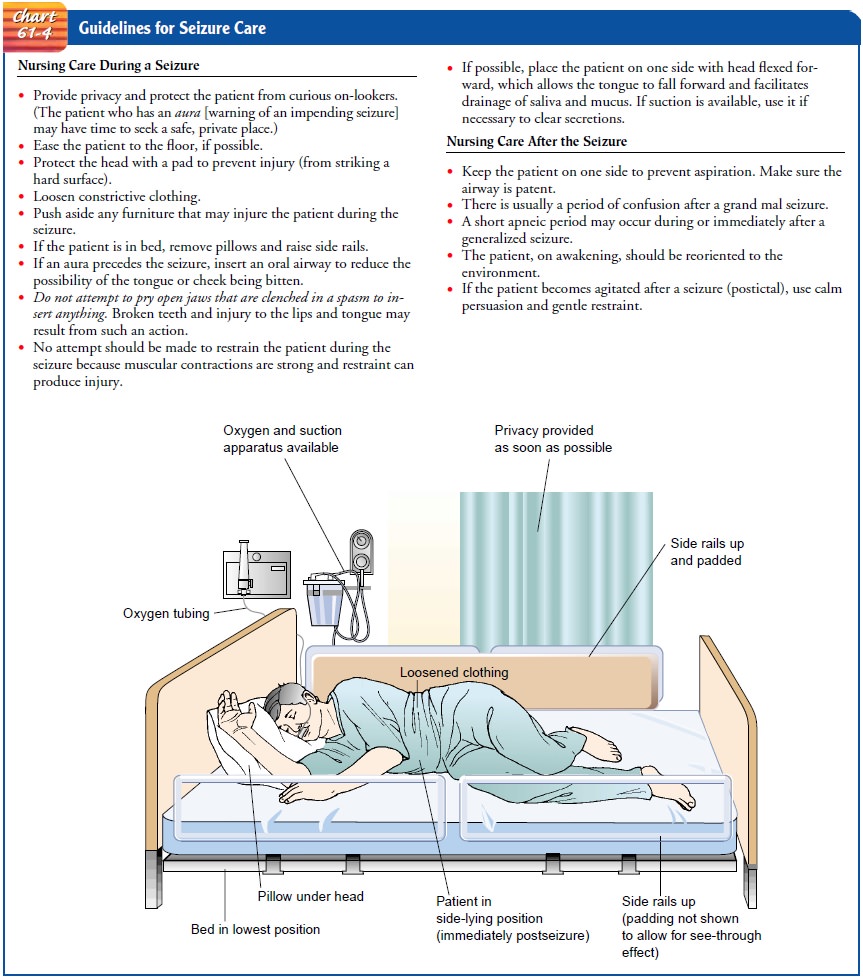
patient (Buelow, 2001). Steps to prevent or minimize injury to the patient are
pre-sented in Chart 61-4.
Nursing Management After a Seizure
After a patient has a seizure, the nurse’s role is
to document the events leading to and occurring during the seizure and to
prevent complications (eg, aspiration, injury). The patient is at risk for
hypoxia, vomiting, and pulmonary aspiration. To prevent com-plications, the
patient is placed in the side-lying position to facil-itate drainage of oral
secretions and is suctioned, if needed, to maintain a patent airway and prevent
aspiration, as described in Chart 61-4. Seizure precautions are maintained,
including having available fully functioning suction equipment with a suction
catheter and oral airway. The bed is placed in a low position with side rails
up and padded if necessary to prevent patient injury. The patient may be drowsy
and may wish to sleep after the seizure; he or she may not remember events
leading up to the seizure and for a short time thereafter.
Related Topics