Chapter: Modern Medical Toxicology: Food Poisons: Food Poisoning
Protozoa - Microbial Food Poisoning
Protozoa
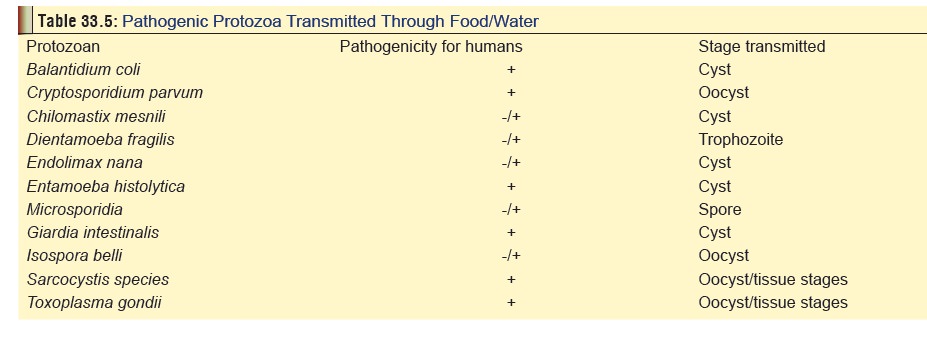
Table 33.5 lists
common protozoa responsible for variouskinds of illnesses that are transmitted
through food and water. While many of these agents are more appropriately
discussed in textbooks of microbiology or clinical medicine, a few merit
special mention here.
Entamoeba histolytica
Source
Contaminated
food and water. Raw vegetables which have not been washed well are an important
source.
Human
to human transmission is also quite common.
Mode of Action
Recent studies have demonstrated
that E. histolytica can be
differentiated into at least 18 zymodemes.* Pathogenic strains are all from
particular zymodemes of which 7 have been iden-tified so far.
Entamoeba histolytica exists in two forms—vegetative(trophozoite) form and cystic form. Trophozoites invade the colon where they multiply and subsequently get encysted. The cysts are excreted in stools. Ingestion of cysts results in release of trophozoites which colonise the large intestine, some of them even invading the bowel wall causing ulcerations.
Occasionally the trophozoites may get transported to other organs such as liver
where they produce abscesses.
Incubation Period
About
2 to 4 weeks
Clinical Features
Entamoeba
histolytica produces a clinical syndrome referredto as amoebiasis, which has a
worldwide distribution and is a major health problem in developing countries.
It is estimated that 15% of the population in India may be affected by amoe-
biasis.
Intestinal
amoebiasis varies in severity from mild abdom- inal discomfort and diarrhoea to
fulminating dysentery. Extra- intestinal amoebiasis may involve liver, lungs,
brain, spleen, etc.
Diagnosis
·
Stool analysis: Microscopy for
detection of trophozoites, cysts, and pus cells.
·
Serological tests: Indirect
haemagglutination test, counter immunoelectrophoresis, ELISA, etc.
Treatment
Symptomatic
cases can be treated with metronidazole (30 mg/ kg/day for 8 to 10 days) or
tinidazole. Abscesses must be treated surgically. Asymptomatic carriers can be
treated (if they are food handlers) with diiodohydroxyquin or diloxanide furoate.
Cryptosporidium parvum
This
protozoon causes severe diarrhoea in immunocompro- mised adult patients and
immunocompetent children.
Source
·
Contaminated food and water,
especially the latter. Decontamination of water can be done by filtration,
distilla- tion, or reverse osmosis.
Clinical Features
1.Severe
persistent diarrhoea.
2.Malnutrition
(in children).
3.Pulmonary
manifestations.
4.Toxic
megacolon.
5.Cryptosporidiosis is often fatal in AIDS patients.
Incubation Period
Biopsy
of intestine (small or large) reveals Haematoxylin and eosin darkly stained
structures 4 to 5 microns in diameter near the tips of microvilli of epithelial
brush border.
Treatment
1.IV
fluids and electrolytes.
2.Antidiarrhoeal
drugs
Microsporidia
The microsporidian genera which
cause human disease include Nosema, Pleistophora, Encephalitozoon,
Enterocytozoon, and Septata.![]()
Microsporidiosis generally occurs
only in immunodeficient patients and can take the form of diarrhoea,
keratoconjunc-tivitis, hepatitis, myositis, ascites, cholangitis, and renal or
urogenital infections. It has been estimated that microsporidia account for 10
to 40% of AIDS-related diarrhoea.
Treatment involves the
administration of albendazole (400 mg twice daily), which helps in relieving
microsporidial diar-rhoea, but relapses are common.
Related Topics