Chapter: Modern Medical Toxicology: Food Poisons: Food Poisoning
Ciguatera Fish Poisoning
Ciguatera Poisoning
Source
Ciguatera poisoning is the commonest
form of seafood poisoning, accounting for more than 50% of the cases.
Barracuda, sea bass, parrot fish, red snapper, grouper, amber- jack, kingfish,
sturgeon, and many other large-sized fish are the main culprits. The following
are associated most commonly with outbreaks of poisoning: grouper (Fig 33.13), parrot fish, surgeon fish,
emperor fish, and red snapper (Fig 33.14).

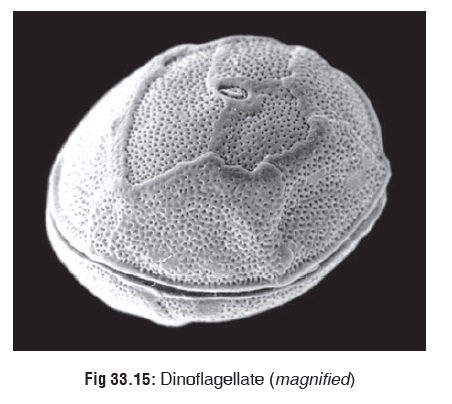
Large fish concentrate the main
toxin (ciguatoxin) due to their food habits. The toxin is present in
dinoflagellates* (Fig33.15), which
are marine protozoa that constitute the main nutritional source for small
herbivorous fish. The latter are in turn consumed by larger carnivorous fish,
and the ciguatoxin ![]() therefore becomes increasingly concentrated (in the flesh, fat, and viscera) of larger and larger fish.
therefore becomes increasingly concentrated (in the flesh, fat, and viscera) of larger and larger fish.
These fish tend to swim close to coral reefs on the ocean’s
bottom in subtropical and tropical latitudes. Ciguatera poisoning is said to be
endemic in the Caribbean, South Pacific, and Australia. A few cases of poisoning
have been reported from some areas of the Indian Ocean also, as well as from
East Asia, and South Asia.
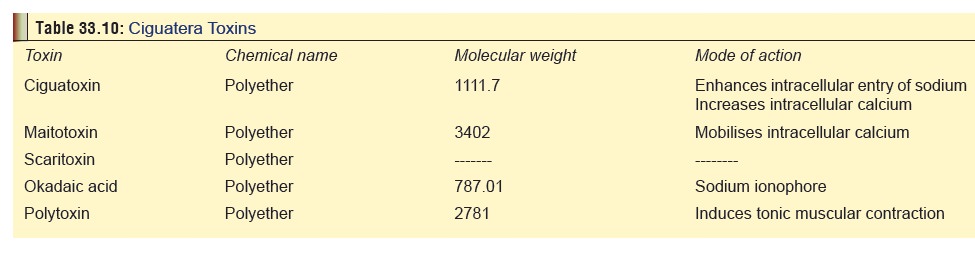
Toxin
Outlined
in Table 33.10, along with mode of
action. The toxins are mainly contained in the muscle, skin and mucosa of the
fish, with the highest concentration present in the viscera (liver, intestines,
gonads).
Incubation Period
About
2 to 6 hours, (range 2 to 24 hours).
Clinical Features
·
Sudden onset of sweating, abdominal cramps, nausea,
vomiting, profuse watery diarrhoea, dysuria, tingling and numbness of lips,
tongue, and throat, metallic taste, paraesthesias, dysaesthesias, chills,
headache, myalgia, arthralgia, tremor, ataxia, vertigo, blurred vision, and
convulsions. Profound weakness may occur. Patients may be unable to rise or move.
Paralysis of limbs and facial muscles may develop in severe cases. Death may
result.
·
Pruritus is frequently reported, and may be mild to severe.
It may persist for weeks after an exposure.
·
Paraesthesias are the hallmark of ciguatera poisoning, and
may also persist for weeks. A characteristic feature is reversal of temperature
discrimination, i.e. cold substances feel hot. But this is not a true sensory
switch; it can be described as the sensation one gets when gripping something
very cold (e.g. ice), and the resultant sensation of a “burning” feeling. These
sensations are usually local-ised to palms, soles, lips and mouth. This
phenomenon is said to be due to abnormal bursts of discharges occurring
specifically in the peripheral C-polymodal nociceptor fibres (cutaneous
afferent unmyelinated fibres). These fibres are not spontaneously active at
normal temperature in undamaged skin, but have a heat threshold above 40°C, and
cold threshold below 23°C. However, contact with heat generally does not
produce the reverse effect.
·
Other sensory effects include a metallic taste, and a
“carbonated” sensation when food or drink is consumed. Teeth may appear loose
and painful.
·
Bradycardia and orthostatic hypotension have also been
reported. Transient T wave inversion has been described. Extrasystoles may
occur, probably because of noradren-ergic myocardial stimulation.
·
Respiratory depression, dyspnoea, and bronchospasm may also
occur.
·
Neurological manifestations tend to linger for a long time
even in patients who have fully recovered.
·
Ocular effects include blurred vision, photophobia, visual
loss (usually temporary), mydriasis and lacrimation.
·
Painful ejaculation and dyspareunia in the unaffected
partner have been reported occasionally.
·
Symptoms of ciguatera poisoning are exacerbated by ethanol
and stress (physical and/or emotional).
·
Foetal distress has occurred after ingestion of
ciguatera-contaminated fish by the pregnant mother. Premature labour and
spontaneous abortion have been reported. Infants exposed to ciguatoxin in late
pregnancy have been noted to have abnormal prenatal movement and temporary
cranial nerve deficits. Several cases of cigua-tera poisoning in breastfeeding
infants whose mothers were poisoned have also been reported.
Diagnosis
·
ELISA test for ciguatoxin.
·
HPLC.
·
A rapid test (dipstick immunobead
assay) is being devel-oped to test suspect fish for the presence of toxin.
Differential Diagnosis
·
Other marine poisonings (scombroid
poisoning, neurotoxic shellfish poisoning) Organophosphate poisoning
·
Monosodium glutamate (in susceptible
individuals)
·
Botulism
·
Other bacterial food poisoning.
Treatment
·
Decontamination (activated charcoal, catharsis) may be of
benefit if the patient is seen within 2 hours of ingestion.
·
The primary treatment is the use of antihistamines; cold
showers can also be helpful. Cyproheptadine may be of benefit.
·
Myalgias usually respond to NSAIDs or other analgesics.
·
Monitor fluid and electrolytes. Monitor vital signs and ECG.
·
Administraton of IV fluids, electrolytes.
·
IV mannitol is said to be useful in the management of
neurological and muscular manifestations. The recom-mended dose is 0.5 to 1
gm/kg of 20% solution, adminis-tered over 30 to 45 minutes. Hypotension may
occur, and must be anticipated whenever mannitol is given. Some investigators
are of the opinion that mannitol is not effec-tive in the management of
neurological manifestations of ciguatera poisoning.
·
Atropine has been of some use in treating bradycardia and
hypotension.
·
Dopamine, plasma expanders, and calcium gluconate may be useful
for shock.
·
Chronic neurologic symptoms may resolve with tocainide,
mexiletine, or amitryptiline.
·
Avoidance of alcohol and exercise (which can exacerbate
symptoms), is recommended.
Related Topics