Chapter: Basic & Clinical Pharmacology : Hypothalamic & Pituitary Hormones
Oxytocin
POSTERIOR PITUITARY HORMONES
The two posterior
pituitary hormones—vasopressin and oxytocin—are synthesized in neuronal cell
bodies in the hypo-thalamus and transported via their axons to the posterior
pituitary, where they are stored and then released into the circulation. Each
has limited but important clinical uses.
OXYTOCIN
Oxytocin is a peptide
hormone secreted by the posterior pituitary that participates in labor and
delivery and elicits milk ejection in lactating women. During the second half
of pregnancy, uterine smooth muscle shows an increase in the expression of
oxytocin receptors and becomes increasingly sensitive to the stimulant action
of endogenous oxytocin. Pharmacologic concentrations of oxytocin powerfully stimulate
uterine contraction.
Chemistry & Pharmacokinetics
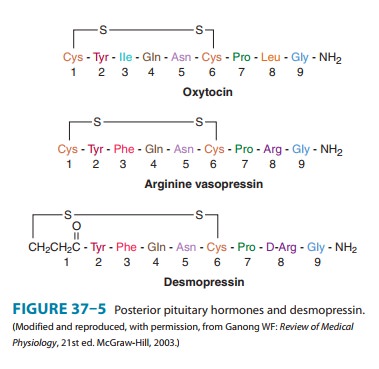
A. Structure
Oxytocin is a
9-amino-acid peptide with an intrapeptide disulfide cross-link (Figure 37–5).
Its amino acid sequence differs from that of vasopressin at positions 3 and 8.
B. Absorption, Metabolism, and Excretion
Oxytocin is
administered intravenously for initiation and aug-mentation of labor. It also
can be administered intramuscularly for control of postpartum bleeding.
Oxytocin is not bound to plasma proteins and is eliminated by the kidneys and
liver, with a circulat-ing half-life of 5 minutes.
Pharmacodynamics
Oxytocin acts through G protein-coupled receptors and the phosphoinositide-calcium second-messenger system to contract uterine smooth muscle. Oxytocin also stimulates the release of prostaglandins and leukotrienes that augment uterine contraction. Oxytocin in small doses increases both the frequency and the force of uterine contractions. At higher doses, it produces sustained contraction.Oxytocin also causes contraction of myoepithelial cells sur-rounding mammary alveoli, which leads to milk ejection. Without oxytocin-induced contraction, normal lactation cannot occur. At high concentrations, oxytocin has weak antidiuretic and pressor activity due to activation of vasopressin receptors.
Clinical Pharmacology
Oxytocin is used to
induce labor for conditions requiring early vaginal delivery such as Rh
problems, maternal diabetes, pre-eclampsia, or ruptured membranes. It is also
used to augment abnormal labor that is protracted or displays an arrest
disorder. Oxytocin has several uses in the immediate postpartum period,
including the control of uterine hemorrhage after vaginal or cesarean delivery.
It is sometimes used during second-trimester abortions.
Before delivery,
oxytocin is usually administered intrave-nously via an infusion pump with
appropriate fetal and maternal monitoring. For induction of labor, an initial
infusion rate of 0.5–2 mU/min is increased every 30–60 minutes until a
physi-ologic contraction pattern is established. The maximum infusion rate is
20 mU/min. For postpartum uterine bleeding, 10–40 units are added to 1 L of 5%
dextrose, and the infusion rate is titrated to control uterine atony.
Alternatively, 10 units of oxytocin can be administered by intramuscular
injection after delivery of the placenta.
During the antepartum
period, oxytocin induces uterine con-tractions that transiently reduce
placental blood flow to the fetus. The oxytocin challenge test measures the
fetal heart rate response to a standardized oxytocin infusion and provides
information about placental circulatory reserve. An abnormal response, seen as
late decelerations in the fetal heart rate, indicates fetal hypoxia and may
warrant immediate cesarean delivery.
Toxicity & Contraindications
When oxytocin is used
judiciously, serious toxicity is rare. The toxicity that does occur is due
either to excessive stimulation of uterine contractions or to inadvertent
activation of vasopressin receptors. Excessive stimulation of uterine
contractions before delivery can cause fetal distress, placental abruption, or
uterine rupture. These complications can be detected early by means of standard
fetal monitoring equipment. High concentrations of oxytocin with activation of
vasopressin receptors can cause excessive fluid retention, or water
intoxication, leading to hyponatremia, heart failure, seizures, and death.
Bolus injections of oxytocin can cause hypotension. To avoid hypotension,
oxy-tocin is administered intravenously as dilute solutions at a con-trolled
rate.
Contraindications to
oxytocin include fetal distress, prematu-rity, abnormal fetal presentation,
cephalopelvic disproportion, and other predispositions for uterine rupture.
Related Topics