Chapter: Basic & Clinical Pharmacology : Hypothalamic & Pituitary Hormones
Hypothalamic & Pituitary Hormones
Hypothalamic & Pituitary
Hormones
The control of
metabolism, growth, and reproduction is mediated by a combination of neural and
endocrine systems located in the hypothalamus and pituitary gland. The
pituitary weighs about 0.6 g and rests at the base of the brain in the bony
sella turcica near the optic chiasm and the cavernous sinuses. The pituitary
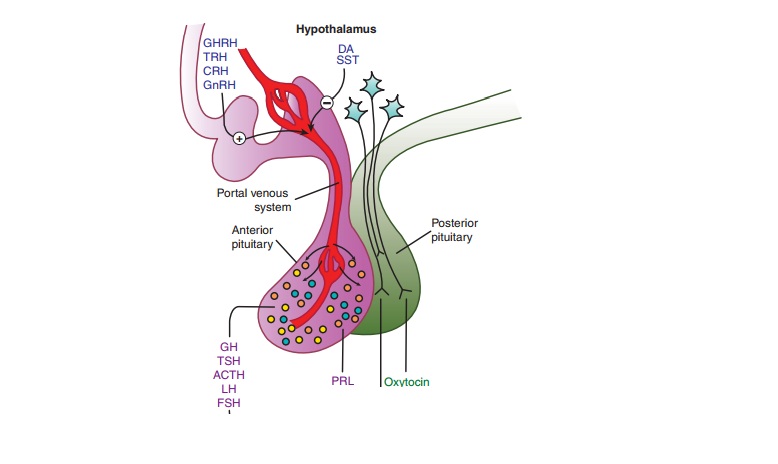
consists of an anterior lobe (adenohypophysis) and a posterior lobe
(neu-rohypophysis) (Figure 37–1). It is connected to the overlying hypothalamus
by a stalk of neurosecretory fibers and blood vessels,including a portal venous
system that drains the hypothalamus and perfuses the anterior pituitary. The
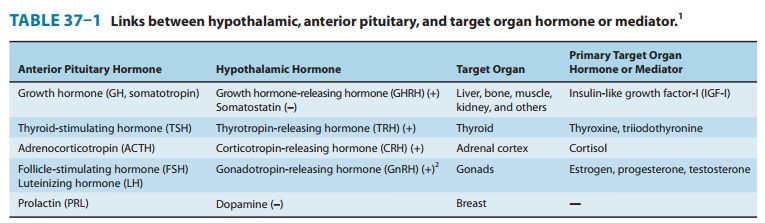
portal venous system car-ries small regulatory hormones (Figure 37–1, Table
37–1) from the hypothalamus to the anterior pituitary.
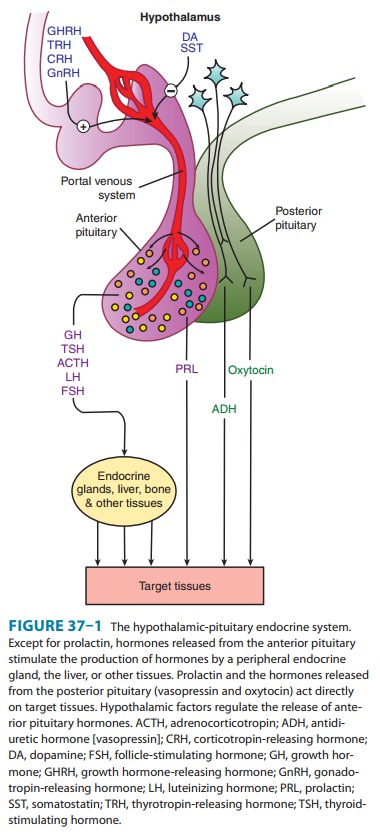
The posterior lobe
hormones are synthesized in the hypothala-mus and transported via the
neurosecretory fibers in the stalk of the pituitary to the posterior lobe, from
which they are released into the circulation.
Drugs that mimic or
block the effects of hypothalamic and pituitary hormones have pharmacologic
applications in three primary areas: (1) as replacement therapy for hormone
deficiency states; (2) as antagonists for diseases caused by excess production
of pituitary hormones; and (3) as diagnostic tools for identifying several
endocrine abnormalities.
CASE STUDY
3-year-old boy [height 85 cm, –3 standard deviations (SD); weight 13 kg, approximately 10th percentile) presents with short stature. Review of the past history and growth chart demonstrates normal birth weight and birth length, but a progressive fall off in height velocity relative to age-matched normal ranges starting at 6 months of age. Physical examination demonstrates short stature and mild general-ized obesity. Genital examination reveals descended but small testes and a phallic length of –2 SD. Laboratory evaluation demonstrates growth hormone (GH) deficiency and a delayed bone age of 18 months. The patient is started on replacement with recombinant human GH at a dose of 40 mcg/kg/d subcutaneously. After 1 year of treatment, his height velocity has increased from 5 cm/yr to 11 cm/yr. How does GH stimulate growth in children? What other hormone deficiencies are suggested by the patient’s physical examination? What other hormone supplementation is this patient likely to require?
CASE STUDY ANSWER
While
GH may have some direct growth-promoting effects, GH is thought to mediate
skeletal growth principally through epiphyseal production of insulin-like
growth factor-I (IGF-I), which acts principally in an autocrine/paracrine
manner. IGF-I may also promote statural growth through endocrine mechanisms.
The findings of small testes and a microphallus in this patient suggest a
diagnosis of hypogonadism, likely as a consequence of gonadotropin deficiency.
This patient is at risk for multiple hypothalamic/pituitary deficiencies. This
patient may already have or may subsequently develop ACTH/ cortisol and
TSH/thyroid hormone deficiencies and thus may require supplementation with
hydrocortisone and levo-thyroxine, in addition to supplementation with GH and
testo-sterone. The patient should also be evaluated for the presence of central
diabetes insipidus and, if present, treated with desmopressin, a V2
vasopressin receptor-selective analog.
Related Topics