Chapter: Basic & Clinical Pharmacology : Nonsteroidal Anti-Inflammatory Drugs, Disease-Modifying Antirheumatic Drugs, Nonopioid Analgesics,& Drugs Used in Gout
Nonsteroidalanti Inflammatory Drugs
NONSTEROIDALANTI INFLAMMATORY DRUGS
Salicylates and other
similar agents used to treat rheumatic disease share the capacity to suppress
the signs and symptoms of inflammation. These drugs also exert antipyretic and
analgesic effects, but it is their anti-inflammatory properties that make them
most useful in the management of disorders in which pain is related to the intensity
of the inflammatory process.Since aspirin, the original NSAID, has a number of
adverse effects, many other NSAIDs have been developed in attempts to improve
upon aspirin’s efficacy and decrease its toxicity.
Chemistry & Pharmacokinetics
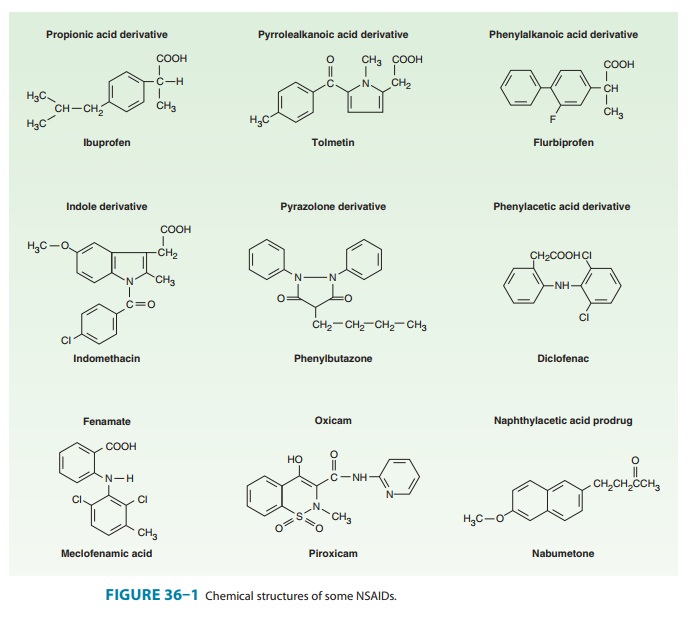
The
NSAIDs are grouped in several chemical classes, as shown in Figure 36–1. This
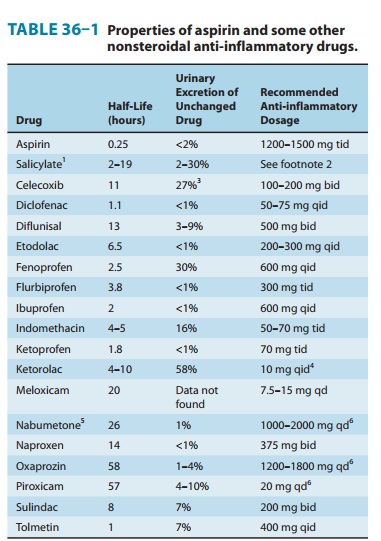
chemical diversity yields a broad range of phar-macokinetic characteristics
(Table 36–1). Although there are many differences in the kinetics of NSAIDs,
they have some gen-eral properties in common. All but one of the NSAIDs are
weak organic acids as given; the exception, nabumetone, is a ketone prodrug
that is metabolized to the acidic active drug.Most of these drugs are well
absorbed, and food does not sub-stantially change their bioavailability. Most
of the NSAIDs are highly metabolized, some by phase I followed by phase II
mecha-nisms and others by direct glucuronidation (phase II) alone. NSAID
metabolism proceeds, in large part, by way of the CYP3A or CYP2C families of
P450 enzymes in the liver. While renal excretion is the most important route
for final elimination, nearly all undergo varying degrees of biliary excretion
and reabsorption (enterohepatic circulation). In fact, the degree of lower
gastroin-testinal (GI) tract irritation correlates with the amount of
entero-hepatic circulation. Most of the NSAIDs are highly protein-bound (∼ 98%), usually to albumin. Most of
the NSAIDs (eg, ibuprofen, ketoprofen) are racemic mixtures, while one,
naproxen, is pro-vided as a single enantiomer and a few have no chiral center
(eg, diclofenac).All NSAIDs can be found in synovial fluid after repeated
dos-ing. Drugs with short half-lives remain in the joints longer than would be
predicted from their half-lives, while drugs with longer half-lives disappear
from the synovial fluid at a rate proportionate to their half-lives.
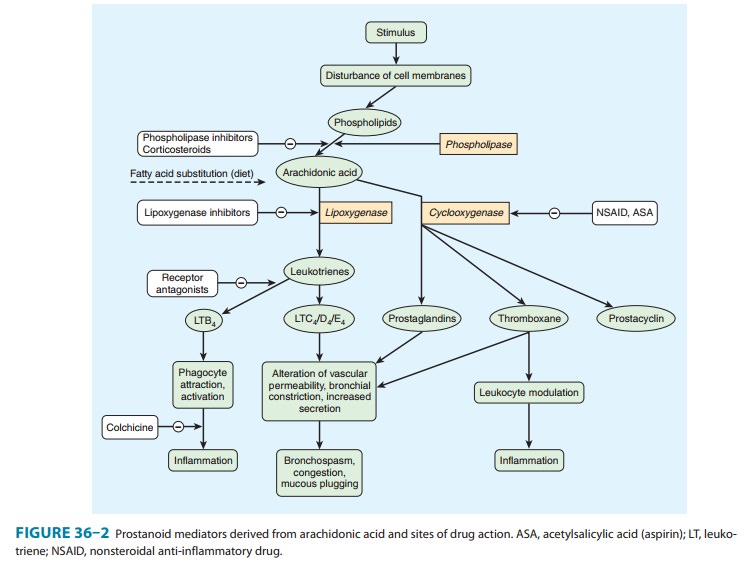
Pharmacodynamics
NSAID
anti-inflammatory activity is mediated chiefly through inhibition of
prostaglandin biosynthesis (Figure 36–2). Various NSAIDs have additional
possible mechanisms of action, including inhibition of chemotaxis, down-regulation
of interleukin-1 pro-duction, decreased production of free radicals and
superoxide, and interference with calcium-mediated intracellular events.
Aspirin irreversibly acetylates and blocks platelet cyclooxygenase, while the
non-COX-selective NSAIDs are reversible inhibitors.
Selectivity
for COX-1 versus COX-2 is variable and incom-plete for the older NSAIDs, but
selective COX-2 inhibitors have been synthesized. The selective COX-2
inhibitors do not affect platelet function at their usual doses. In testing
using human whole blood, aspirin, ibuprofen, indomethacin, piroxicam, and
sulindac are somewhat more effective in inhibiting COX-1. The efficacy of
COX-2-selective drugs equals that of the older NSAIDs, while GI safety may be
improved. On the other hand, selective COX-2 inhibitors may increase the
incidence of edema and hypertension. As of August 2011, celecoxib and the less
selec-tive meloxicam were the only COX-2 inhibitors marketed in the USA.
Rofecoxib and valdecoxib, two previously marketed, selec-tive COX-2 inhibitors,
were withdrawn from the market because of their association with increased
cardiovascular thrombotic events. Celecoxib has a Food and Drug Administration
initiated “black box” warning concerning cardiovascular risks. It has been recommended
that all NSAID product labels be revised to men-tion cardiovascular risks.
The NSAIDs decrease the sensitivity of vessels to bradykinin and histamine, affect lymphokine production from T lympho-cytes, and reverse the vasodilation of inflammation. To varying degrees, all newer NSAIDs are analgesic, anti-inflammatory, and antipyretic, and all (except the COX-2-selective agents and the nonacetylated salicylates) inhibit platelet aggregation. NSAIDs are all gastric irritants and can be associated with GI ulcers and bleeds as well, although as a group the newer agents tend to cause less GI irritation than aspirin. Nephrotoxicity has been observed for all of the drugs for which extensive experience has been reported.
Nephrotoxicity is due,
in part, to interference with the autoregula-tion of renal blood flow, which is
modulated by prostaglandins. Hepatotoxicity can also occur with any NSAID.
Although
these drugs effectively inhibit inflammation, there is no evidence that—in
contrast to drugs such as methotrexate and other DMARDs—they alter the course
of any arthritic disorder.
Several
NSAIDs (including aspirin) reduce the incidence of colon cancer when taken
chronically. Several large epidemiologic studies have shown a 50% reduction in
relative risk when the drugs are taken for 5 years or longer. The mechanism for
this protective effect is unclear.
The
NSAIDs have a number of commonalities. Although not all NSAIDs are approved by
the FDA for the whole range of rheumatic diseases, most are probably effective
in rheumatoid arthritis, sero-negative spondyloarthropathies (eg, psoriatic
arthritis and arthritis associated with inflammatory bowel disease),
osteoarthritis, local-ized musculoskeletal syndromes (eg, sprains and strains,
low back pain), and gout (except tolmetin, which appears to be ineffec-tive in
gout).
Adverse
effects are generally quite similar for all of the NSAIDs:
1. Central nervous system: Headaches, tinnitus, and dizziness.
2. Cardiovascular: Fluid retention, hypertension, edema, andrarely, myocardial
infarction, and congestive heart failure.
3. Gastrointestinal: Abdominal pain, dysplasia, nausea, vomit-ing, and rarely, ulcers
or bleeding.
4. Hematologic: Rare thrombocytopenia, neutropenia, or evenaplastic anemia.
5. Hepatic: Abnormal liver function tests and rare liver failure.
6. Pulmonary: Asthma.
7. Skin: Rashes, all types, pruritus.
8. Renal: Renal insufficiency, renal failure, hyperkalemia,
andproteinuria.
Related Topics