Chapter: Basic & Clinical Pharmacology : Nonsteroidal Anti-Inflammatory Drugs, Disease-Modifying Antirheumatic Drugs, Nonopioid Analgesics,& Drugs Used in Gout
Colchicine
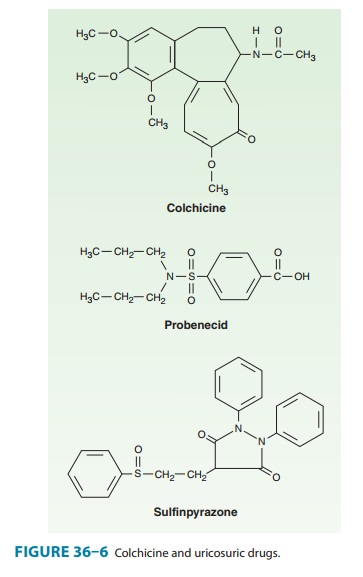
COLCHICINE
Although NSAIDs are
now the first-line drugs for acute gout, colchicine was the primary treatment
for many years. Colchicine is an alkaloid isolated from the autumn crocus, Colchicumautumnale. Its structure is
shown in Figure 36–6.
Pharmacokinetics
Colchicine is absorbed readily after oral administration, reaches peak plasma levels within 2 hours, and is eliminated with a serum half-life of 9 hours. Metabolites are excreted in the intestinal tract and urine.
Pharmacodynamics
Colchicine relieves
the pain and inflammation of gouty arthritis in 12–24 hours without altering
the metabolism or excretion of urates and without other analgesic effects.
Colchicine produces its anti-inflammatory effects by binding to the
intracellular protein tubulin, thereby preventing its polymerization into
microtubules and leading to the inhibition of leukocyte migration and
phago-cytosis. It also inhibits the formation of leukotriene B4. Several of
colchicine’s adverse effects are produced by its inhibition of tubulin
polymerization and cell mitosis.
Indications
Although colchicine is
more specific in gout than the NSAIDs, NSAIDs (eg, indomethacin and other
NSAIDs [except aspirin]) are sometimes used in its stead because of the
troublesome diarrhea associated with colchicine therapy. Colchicine is now used
between attacks (the “intercritical period”) for prolonged prophylaxis (at low
doses). It is effective in preventing attacks of acute Mediterranean fever and
may have a mild beneficial effect in sarcoid arthritis and in hepatic
cirrhosis. (Although it has been
givenintravenously, this route is no longer approved by the FDA [2009].)
Adverse Effects
Colchicine
often causes diarrhea and may occasionally cause nau-sea, vomiting, and
abdominal pain. Hepatic necrosis, acute renal failure, disseminated
intravascular coagulation, and seizures have also been observed. Colchicine may
rarely cause hair loss and bone marrow depression, as well as peripheral
neuritis, myopathy, and, in some cases, death. The more severe adverse events
have been associated with the intravenous administration of colchicine. Acute
overdose is characterized by burning throat pain, bloody diarrhea, shock, hematuria,
and oliguria. Fatal ascending central nervous system depression has been
reported. Supportive care is the mainstay of treatment.
Dosage
In
prophylaxis (the most common use), the dosage of colchicine is 0.6 mg one to
three times daily. For terminating a gouty attack, traditional dosing has been
an initial colchicine dose of 0.6 or 1.2 mg, followed by 0.6 mg every 2 hours
until pain resolves, or nau-sea and diarrhea appear. However, a regimen of 1.2
mg followed by a single 0.6 mg oral dose was shown to be as effective as the
higher dose therapy noted above. Adverse events were less with this lower dose
regimen. In February 2008, the FDA requested that intravenous preparations
containing colchicine be discontin-ued in the USA because of their potential life-threatening
adverse effects. Therefore, intravenous use of colchicine is not recom-mended.
In July 2009, the FDA
approved colchicine for the treatment of acute gout, allowing Colcrys (a
branded colchicine) marketing exclusivity in the USA. Colchicine, per se,
rather than Colcrys, is available throughout the rest of the world in a generic
form.
Related Topics