Chapter: Medicine and surgery: Genitourinary system
Mesangiocapillary glomerulonephritis (membranoproliferative GN) - Glomerular disease
Mesangiocapillary glomerulonephritis (membranoproliferative GN)
Definition
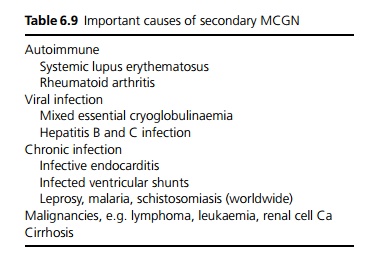
MCGN (or MPGN) is a descriptive term for a pattern of glomerular disease with mesangial proliferation and GBM thickening. It may be a primary disease (two types) but many cases are secondary (see Table 6.9).
Aetiology/pathophysiology
Type I MCGN is almost certainly an immune complex mediated disease, perhaps caused by an unknown infectious agent.
Type II MCGN is also called ŌĆśdense deposit diseaseŌĆÖ because on electron microscopy, continuous ribbon like deposits of C3 are seen along the GBM, tubules and BowmanŌĆÖs capsule. The cause is unknown, but there is an association with partial lipodystrophy.
In type I, immune complexes activate complement, whereas in type II there is increased peripheral consumption of C3 by a circulating IgG antibody (C3nephritic factor).
Clinical features
Patients usually present with haematuria and/or proteinuria and a variable degree of renal failure. In severe cases patients may present with nephrotic syndrome, nephritic syndrome or a mixed picture. Features of any underlying condition may also be present.
Investigations
Renal biopsy is required for diagnosis. Low C3, with normal C1q and C4. C3 nephritic factor positive in MCGN type II. Underlying causes should be looked for, particularly treatable infections, malignancies and cryoglobulinaemia.
Management
Treatment of any underlying cause may lead to partial or complete remission. In those without nephrotic syndrome, conservative management is probably indicated, as the prognosis is good. In those with nephroticrange proteinuria, specific treatments such as steroids and antiplatelet agents may be tried with very variable benefit.
Prognosis
Idiopathic MCGN is typically progressive leading to end stage renal failure. It often recurs in transplanted kidneys.
Related Topics