Chapter: Medicine and surgery: Genitourinary system
Acute tubular necrosis (ATN) - Disorders of the kidney
Acute tubular necrosis (ATN)
Definition
Necrosis of renal tubular epithelium as caused by hypoperfusion of the kidneys and certain toxins.
Aetiology
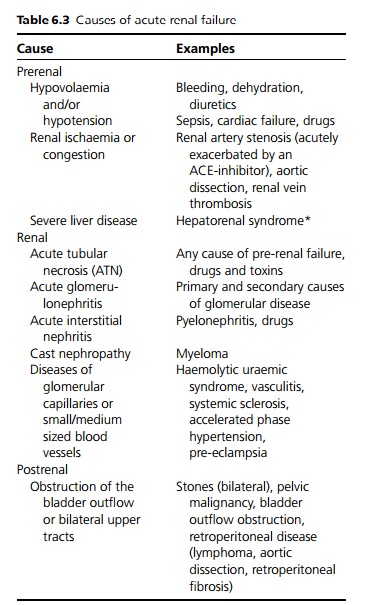
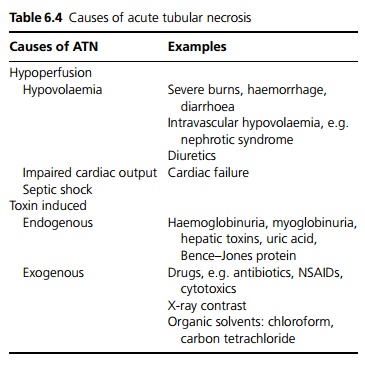
The main causes are hypoperfusion, i.e. the causes of prerenal failure (more common) and toxins (see Tables 6.3 and 6.4).
Pathophysiology
The renal medulla is particularly susceptible to is-chaemia, because of high metabolic activity. In addition, in shock renal blood flow is particularly likely to suffer because of constriction of renal vessels due to sympathetic activity and the release of vasoconstrictive substances. The glomerular filtration rate (GFR) falls in response to hypoperfusion, and ischaemia causes the tubules to lose function.
Toxins may have a variety of mechanisms such as causing vasoconstriction, a direct toxic effect on tubular cells causing their dysfunction, and they may also cause the death of tubular epithelial cells which block the tubules. The glomeruli (which are well perfused) may continue to filter urine in large volumes, and if the tubules are not reabsorbing the filtrate, urine output may be maintained (non-oliguric renal failure) or even increased (polyuric renal failure).
Ischaemia or toxins can cause tubular epithelial cells to die and slough away from the basement membrane, blocking the tubules. Blockage of the renal tubules causes a secondary reduction in glomerular blood flow.
If the basement membrane is intact, tubular epithelium regrows within 10–20 days, restoring function to the nephrons. Dead material is phagocytosed. The epithelial cells take time to differentiate and develop their concentrating function.
Clinical features
ATN presents as with acute renal failure. It typically passes through three phases:
· Oliguric phase (reduced GFR): Acute renal failure with complications of hyperkalaemia, metabolic acidosis and fluid overload (pulmonary oedema). This phase may last many weeks, depending on the initial severity of insult.
· Polyuric phase: This is during early recovery, patients may pass 5 L or more of urine a day and are at risk of developing secondary problems with water and electrolyte (Na+ , K+ , Ca++ ) depletion. Initially uraemia may persist, but this usually gradually improves.
· Recovery to baseline renal function, or with some residual deficit.
Management
The management is similar to that of acute renal failure.
Prognosis
In acute tubular necrosis the mortality is high but if the patient survives the prognosis for renal recovery is good.
Related Topics