Chapter: Medicine and surgery: Genitourinary system
Measuring renal function - Investigations and procedures
Measuring renal function
Renal function testing involves measuring urea and creatinine and
glomerular filtration rate (GFR). Urea and creatinine may remain normal until
more than half of renal function is lost.
Normal kidneys receive 25% of the cardiac output. The volume that is
ultrafiltrated per minute is the GFR, and it is the sum of the filtration that
occurs in all the functioning nephrons. When nephrons are lost or are not
functioning properly, there is compensation by the remaining nephrons by
hyperfiltration, and improved solute clearance. If there is poor blood supply
to the kidneys, due for example to hypotension or cardiac failure, the GFR will
fall ŌĆō even though the nephrons are intact.
Serum urea: Urea is freely filtered at the glomeruli, but variably reabsorbed by the tubules, and its production fluctuates
considerably, even within an individual. It is higher following protein intake,
in a catabolic state, after steroids or gastrointestinal (GI) haemorrhage, and
lower when patients are not eating, and in liver disease. In dehydration, urea
rises proportionally more than creatinine because it is avidly reabsorbed at
the proximal tubules in a fluid-depleted state.
A urea above normal therefore suggests renal failure, GI bleeding or
dehydration. If the creatinine is also proportionally raised (creatinine is
normally Ōł╝20├Ś urea) above normal, this indicates intrinsic renal failure.
Serum creatinine: Creatinine is produced as a waste
product when creatine phosphate is broken down in muscle. The amount
produced is lower in those with low muscle bulk, in women, children and the
elderly. It is freely filtered, a small amount is also secreted at the tubules.
Plasma creatinine is increased by strenuous exercise, ingestion of meat,
certain drugs (trimethoprim and cimetidine) impair tubular secretion. It is
decreased in malnutrition, wasting diseases, immediately after surgery and by
corticosteroids. For these reasons there is wide variation in normal creatinine
levels between individuals. In most patients, serial or previous measurements
of creatinine are useful to monitor the progress of renal function.
Glomerular filtration rate (GFR):
To assess the GFR the rate at which a substance is cleared from the plasma is measured.
The normal GFR = 80ŌĆō130 mL/min/1.73 m2 body surface area. Clearance is
defined as the ŌĆśvirtualŌĆÖ volume of blood cleared (by the kidney) of solute per
unit time. If a substance is completely filtered by the glomeruli and not
secreted, absorbed or metabolised by the renal tubules then its urinary
clearance equals GFR. Creatinine almost fulfils these criteria, and is used in
clinical practice to measure GFR using a 24-hour urine collection:

where U = urinary concentration, V = urine flow rate and P = plasma creatinine.
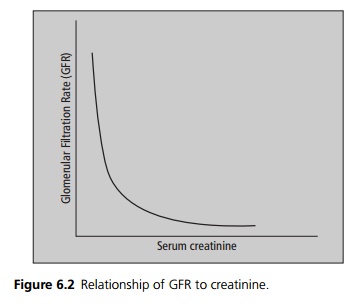
Blood creatinine levels are inversely related to clearance. This means
that with normal renal function a small rise in creatinine means a large fall
in GFR. Conversely in patients with moderate to severe renal failure, i.e. a
low GFR, even a small further fall in GFR will result in a large increase in
creatinine (see Fig. 6.2).
24-hour urinary collections are inconvenient and inaccurate. The
creatinine clearance can be calculated from a patientŌĆÖs serum creatinine using
formulae correcting for factors like the patientŌĆÖs age, sex and weight (which
adjust for muscle mass). The best known of these is the Cockcroft and Gault
formula:

For women multiply by 1.04 rather than 1.23. When accurate GFR measurement is needed the rate of clearance of a radioisotope is used. This is indicated in severe renal failure (creatinine clearance becomes inaccurate), for kidney donors and patients receiving chemotherapy.
Related Topics