Chapter: Biology of Disease: Transfusion and Transplantation
Immunosuppression
IMMUNOSUPPRESSION
All patients who receive an allograft are liable to
reject the transplant, even if the recipient and host are closely matched for
histocompatibility antigens. This is because relatively few of the HLA antigens
are tested for, and complete matches are rare. Thus, all patients who receive
an allograft have to take immu-nosuppressive drugs to prevent rejection resulting
from an immune response. Immunosuppressive treatments fall into a number of
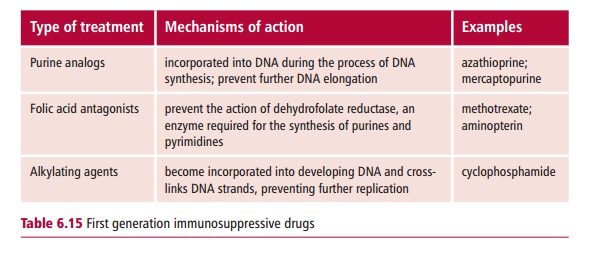
categories. The first gen-eration of immunosuppressive drugs were used to
prevent lymphocytes from proliferating (Table
6.15). As these drugs act by inhibiting cell division, they are also used
in the treatment of cancer. Their actions are described. Corticosteroids, such
as cortisol, are also immunosup-pressive agents but act principally by
suppressing inflammation. They are still used, often in combination with other
drugs such as methotrexate. All the first generation drugs produce a ‘blanket’
immunosuppression and prevent all immune responses. This makes the patient more
susceptible to infections of all kinds, but especially to opportunistic
infections caused by such organisms as Candida
albicans. Immunosuppressed patients are also more susceptible to the types
of cancers associated with viruses, including lymphoma, associ-ated with the
Epstein-Barr virus (EBV) and Kaposi’s sarcoma, associated with the Kaposi’s
sarcoma associated herpes virus (KSV). First generation immu-nosuppressive
treatments also have significant toxicity, because they affect all dividing
cells, including those of the bone marrow and of the GIT. Some, such as
methotrexate, also show liver toxicity.
The second generation of immunosuppressive treatments
target T lym-phocytes rather than B cells. These included the use of
antilymphocyte globulin, an antibody raised against human T lymphocytes. The
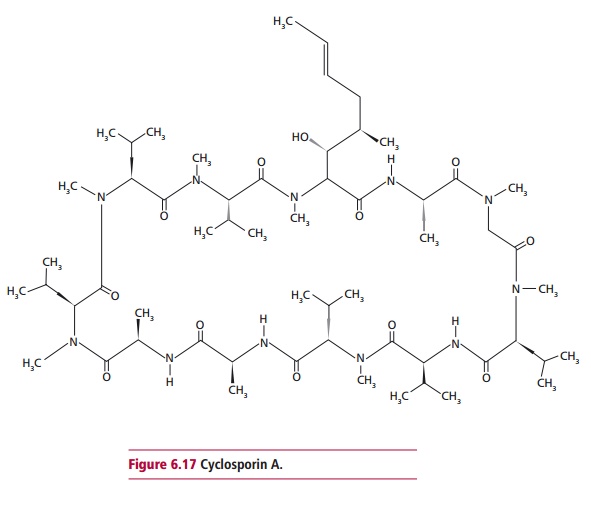
third gen-eration of immunosuppressive treatments are much more selective in
their action and target only those T cells which have been activated by an
antigen. Cyclosporin A, a cyclic peptide (Figure
6.17) derived from the soil fungus Tolypocladium
inflatum gams, is most commonly used. The peptide showsconsiderable
immunosuppressive action, without the bone marrow toxic-ity demonstrated by
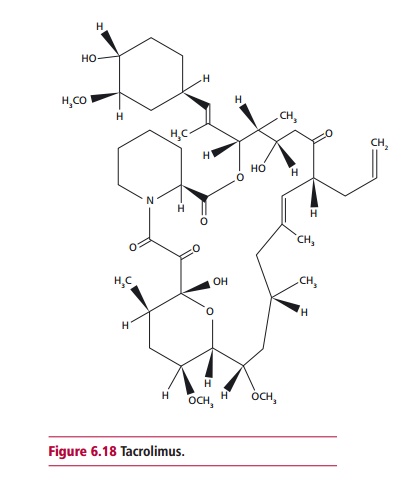
other drugs. Tacrolimus, a macrolide antibiotic (Figure6.18) derived from
Streptomyces tsukubaensis, is similar to cyclosporin A inaction. It is more
powerful than cyclosporin A but also has more side effects. Mycophenolate
mofetil is an example of a prodrug, which is converted in the body to
mycophenolic acid, another powerful immunosuppressive agent.
Related Topics