Chapter: Clinical Anesthesiology: Perioperative & Critical Care Medicine: Management of Patients with Fluid & Electrolyte Disturbances
Hypomagnesemia
HYPOMAGNESEMIA
Hypomagnesemia is a common and frequently
overlooked problem, particularly in critically ill patients, and is often
associated with deficiencies of other intracellular components such as
potassium and phosphorus. It is commonly found in patients undergoing major
cardiothoracic or abdominal operations, and its incidence among patients in
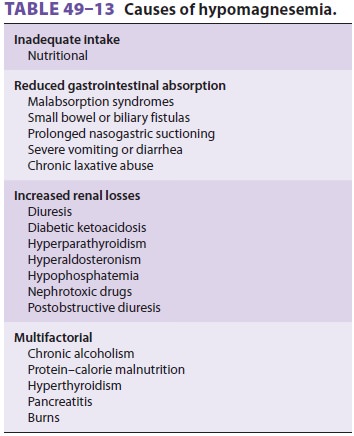
intensive care units may exceed 50%. Deficiencies of magnesium are generally
the result of inadequate intake, reduced gastrointestinal absorption, and
increased renal excretion ( Table 49–13).
Drugs that cause renal wasting of magnesium include ethanol, theophylline,
diuretics, cisplatin, aminoglycosides, cyclosporine, amphotericin B,
pentamidine, and granulocyte colony-stimulating factor.
Clinical Manifestations of Hypomagnesemia
Most patients with hypomagnesemia are asymp-tomatic, but anorexia,
weakness, fasciculation, par-esthesias, confusion, ataxia,
and seizures may be encountered. Hypomagnesemia is frequently associ-ated with both
hypocalcemia (impaired PTH secre-tion) and hypokalemia (due to renal K
wasting). Cardiac manifestations include electrical irritability and
potentiation of digoxin toxicity; both factors are aggravated by hypokalemia.
Hypomagnesemia is associated with an increased incidence of atrial
fibrillation. Prolongation of the P–R and QT inter-vals may also be present.
Treatment of Hypomagnesemia
Asymptomatic hypomagnesemia can be treated orally or intramuscularly.
Serious manifestations such as seizures should be treated with intravenous
magnesium sulfate, 1–2 g (8–16 mEq or 4–8 mmol) given slowly over 15–60 min.
Anesthetic Considerations
Although no specific anesthetic interactions
are described, coexistent electrolyte disturbances such as hypokalemia, hypophosphatemia,
and hypocalce-mia are often present and should be corrected prior to surgery. Isolated hypomagnesemia should be corrected prior to
elective proceduresbecause of its potential for causing cardiac
arrhyth-mias. Moreover, magnesium appears to have intrin-sic antiarrhythmic
properties and possibly cerebral protective effects . It is frequently
administered preemptively to lessen the risk of post-operative atrial
fibrillation in patients undergoing cardiac surgery.
Related Topics