Chapter: Basic & Clinical Pharmacology : Drugs Used in the Treatment of Gastrointestinal Diseases
Drugs Stimulating Gastrointestinal Motility
DRUGS STIMULATING GASTROINTESTINAL
MOTILITY
Drugs that can
selectively stimulate gut motor function (prokinetic
agents) have significant potential clinical usefulness. Agents that increase
lower esophageal sphincter pressures may be useful for GERD. Drugs that improve
gastric emptying may be helpful for gastroparesis and postsurgical gastric
emptying delay. Agents that stimulate the small intestine may be beneficial for
postoperative ileus or chronic intestinal pseudo-obstruction. Finally, agents
that enhance colonic transit may be useful in the treatment of consti-pation.
Unfortunately, only a limited number of agents in this group are available for
clinical use at this time.
PHYSIOLOGY OF THE ENTERIC NERVOUS SYSTEM
The enteric nervous
system is composed of interconnected
networks of ganglion cells and nerve fibers mainly located in the submucosa
(submucosal plexus) and between the circular and longitudinal muscle layers
(myenteric plexus). These networks give rise to nerve fibers that connect with
the mucosa and muscle. Although extrinsic sympathetic and parasympathetic nerves
project onto the submucosal and myenteric plexuses, the entericnervous system
can independently regulate gastrointestinal motility and secretion. Extrinsic
primary afferent neurons project via the dorsal root ganglia or vagus nerve to
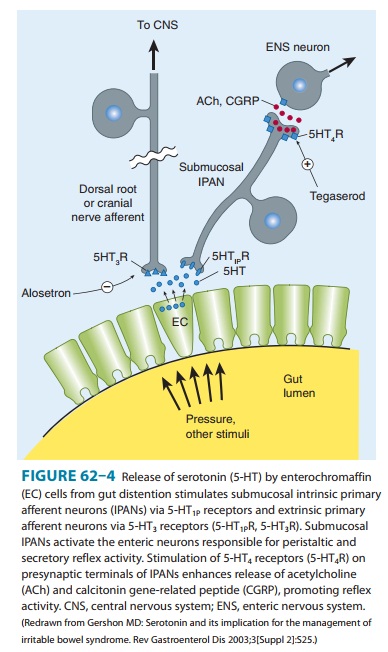
the central nervous system (Figure 62–4). Release of serotonin (5-HT) from
intestinal mucosa enterochromaffin (EC) cells stimulates 5-HT3 receptors on the
extrinsic afferent nerves, stimulating nausea, vomiting, or abdomi-nal pain.
Serotonin also stimulates submucosal 5-HT1P receptors of the intrinsic primary afferent
nerves (IPANs), which contain calci-tonin gene-related peptide (CGRP) and
acetylcholine and project to myenteric plexus interneurons. 5-HT4 receptors on the
presynaptic terminals of the IPANs appear to enhance release of CGRP or
ace-tylcholine. The myenteric interneurons are important in controlling the
peristaltic reflex, promoting release of excitatory mediators proximally and
inhibitory mediators distally. Motilin may stimulate excitatory neurons or
muscle cells directly. Dopamine acts as an inhibitory neurotransmitter in the
gastrointestinal tract, decreasing the intensity of esophageal and gastric
contractions.
Although
there are at least 14 serotonin receptor subtypes, 5-HT drug development for
gastrointestinal applications to date has focused on 5-HT3-receptor antagonists and 5-HT4-receptoragonists. These
agents—which have effects on gastrointestinalmotility and visceral afferent
sensation—are discussed under Drugs Used for the Treatment of Irritable Bowel
Syndrome and Antiemetic Agents.
CHOLINOMIMETIC AGENTS
Cholinomimetic
agonists such as bethanechol stimulate muscarinic M3 receptors on muscle
cells and at myenteric plexus synapses . Bethanechol was used in the past for
the treatment of GERD and gastroparesis. Owing to multiple cholinergic effects
and the advent of less toxic agents, it is now seldom used. The
acetylcholinesterase inhibitor neostigmine can enhance gastric, small
intestine, and colonic emptying. Intravenous neostigmine has enjoyed a
resurgence in clinical usage for the treatment of hos-pitalized patients with
acute large bowel distention (known as acute colonic pseudo-obstruction or
Ogilvie’s syndrome). Administration of 2 mg results in prompt colonic
evacuation of flatus and feces in the majority of patients. Cholinergic effects
include excessive sali-vation, nausea, vomiting, diarrhea, and bradycardia.
METOCLOPRAMIDE & DOMPERIDONE
Metoclopramide
and domperidone are dopamine D2-receptor
antagonists. Within the gastrointestinal tract activation of dop-amine
receptors inhibits cholinergic smooth muscle stimulation; blockade of this
effect is believed to be the primary prokinetic mechanism of action of these
agents. These agents increase esoph-ageal peristaltic amplitude, increase lower
esophageal sphincter pressure, and enhance gastric emptying but have no effect
on small intestine or colonic motility. Metoclopramide and domperi-done also
block dopamine D2 receptors
in the chemoreceptor trigger zone of the medulla (area postrema), resulting in
potent antinausea and antiemetic action.
Clinical Uses
A. Gastroesophageal Reflux Disease
Metoclopramide is
available for clinical use in the USA; domperi-done is available in many other
countries. These agents are some-times used in the treatment of symptomatic
GERD but are not effective in patients with erosive esophagitis. Because of the
supe-rior efficacy and safety of antisecretory agents in the treatment of
heartburn, prokinetic agents are used mainly in combination with antisecretory
agents in patients with regurgitation or refractory heartburn.
B. Impaired Gastric Emptying
These
agents are widely used in the treatment of patients with delayed gastric
emptying due to postsurgical disorders (vagotomy, antrectomy)and diabetic
gastroparesis. Metoclopramide is sometimes adminis-tered in hospitalized
patients to promote advancement of nasoenteric feeding tubes from the stomach
into the duodenum.
C. Nonulcer Dyspepsia
These agents lead to
symptomatic improvement in a small num-ber of patients with chronic dyspepsia.
D. Prevention of Vomiting
Because of their
potent antiemetic action, metoclopramide and domperidone are used for the
prevention and treatment of emesis.
E. Postpartum Lactation Stimulation
Domperidone is
sometimes recommended to promote postpartum lactation (see also Adverse
Effects).
Adverse Effects
The
most common adverse effects of metoclopramide involve the central nervous
system. Restlessness, drowsiness, insomnia, anxiety, and agitation occur in
10–20% of patients, especially the elderly. Extrapyramidal effects (dystonias,
akathisia, parkinsonian features) due to central dopamine receptor blockade
occur acutely in 25% of patients given high doses and in 5% of patients receiving
long-term therapy. Tardive dyskinesia, sometimes irreversible, has devel-oped
in patients treated for a prolonged period with metoclopramide. For this
reason, long-term use should be avoided unless absolutely necessary, especially
in the elderly. Elevated prolactin levels (caused by both metoclopramide and
domperidone) can cause galactor-rhea, gynecomastia, impotence, and menstrual
disorders.
Domperidone
is extremely well tolerated. Because it does not cross the blood-brain barrier
to a significant degree, neuropsychi-atric and extrapyramidal effects are rare.
MACROLIDES
Macrolide
antibiotics such as erythromycin
directly stimulate motilin receptors on gastrointestinal smooth muscle and
promote the onset of a migrating motor complex. Intravenous erythromycin (3
mg/kg) is beneficial in some patients with gastroparesis; how-ever, tolerance
rapidly develops. It may be used in patients with acute upper gastrointestinal
hemorrhage to promote gastric emp-tying of blood before endoscopy.
Related Topics