Chapter: Essential Anesthesia From Science to Practice : Applied physiology and pharmacology : A brief pharmacology related to anesthesia
Antiarrhythmic drugs
Antiarrhythmic drugs (Table 12.16)
Peri-operatively,
we see more tachycardias (light anesthesia) than bradycardias (which might be
an ominous sign of profound hypoxemia or in children an indi-cation of all too
deep anesthesia), and we treat them according to their etiologies. That is, we
would not give beta blockers to reduce heart rate if light anesthesia must be
held responsible for the rapid rate, nor would we give atropine to treat
hypoxemia-induced bradycardia.
For the
treatment of arrhythmias of the atria and ventricles, we have a large selection
of fairly specific drugs from which we have picked a few that find frequent use
in anesthesia and/or cardiac life support (Table 12.16).
Both atropine and glycopyrrolate can be used to treat symptomatic bradycardia.
However, in patients with acute myocardial ischemia, raising the heart rate can
be dangerous because it will increase oxygen demand.
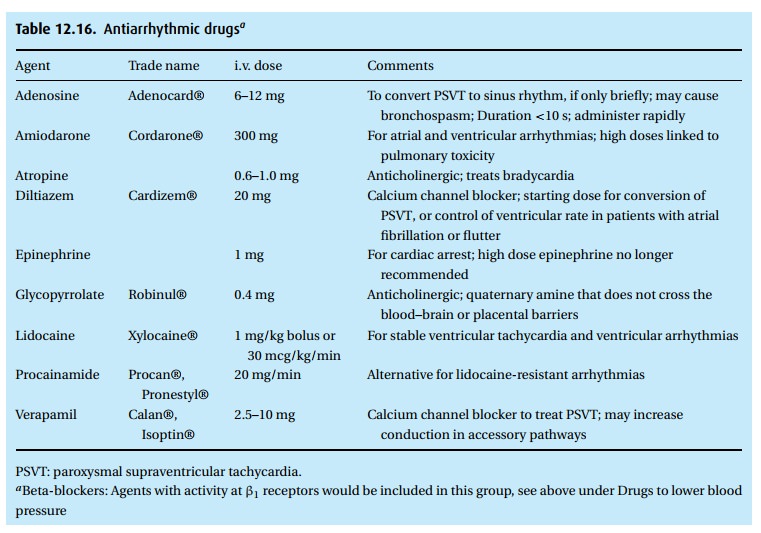
Adenosine
as a drug occupies a special niche because the body itself synthesizes this
fleeting byproduct of ATP. We use it primarily in the treatment of re-entrant
AV node tachycardias such as paroxysmal supraventricular tachycardia (PSVT).
Even if the rhythm fails to convert to sinus, the transient slowing of the
tachycardia can help with a specific diagnosis.
Lidocaine
and procainamide work not only as local anesthetics (lidocaine bet-ter than
procainamide) but also as useful antiarrhythmic drugs in the treatment of
ventricular extrasystoles. Two calcium channel blockers deserve mention:
dilti-azem and verapamil. Both find use in the treatment of a variety of
supraventricular arrhythmias and by slowing AV conduction, they can reduce
heart rate in patients in atrial fibrillation.
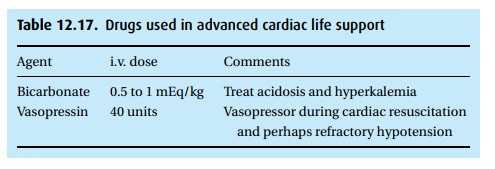
Advanced cardiac life support
Many
drugs already discussed also appear in manuals on cardiac life support, for
example in the treatment of arrhythmias and hypotension. The two drugs
presented in Table 12.17not yet mentioned
deserve a brief note. In the past, sodium bicarbonate was given in cardiac
arrest probably more often than useful. Currently, the American Heart
Association recommends it for the treatment of pre-existing hyperkalemia, in
diabetic ketoacidosis, in patients overdosed with tricyclic antidepressants or
cocaine, and to alkalinize the urine in aspirin poison-ing. We usually start
with 1 mEq/kg and then, if possible, check arterial blood gases before giving
more. Vasopressin, a relatively new addition to the list of drugs used in
advanced cardiac life support, powerfully constricts vessels. A single dose of
40 units has been used instead of epinephrine in patients in ventricular
fibrillation who had failed to respond to three shocks.
Related Topics