Chapter: Medicine and surgery: Hepatic, biliary and pancreatic systems
Alcohol-induced liver disease
liver diseases
Alcohol-induced liver disease
Definition
Liver disease caused by alcohol range from a fatty liver to hepatitis and cirrhosis.
Incidence/prevalence
Alcohol is the most common cause of liver disease in the West.
Geography
Increasing importance in developing countries.
Aetiology
The risk of developing chronic disease is related to quantity, types of beverage, drinking pattern, nutrition and genetic susceptibility.
Pathophysiology
Any alcohol ingestion causes changes in liver cells, which can be seen by electron microscopy. Alcoholic hepatitis refers to alcohol-induced liver injury visible by light microscopy. Alcohol may alter and/or enhance the effects of other chemicals on the liver, including other hepatotoxins and carcinogens.
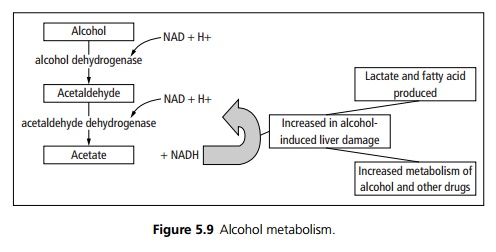
Alcohol increases lactate and fatty acid accumulation resulting in fatty liver.
Chronic alcohol use activates the microsomal oxidising system, which increases metabolism of alcohol and other drugs (see Fig. 5.9). Cirrhosis may result from fibroblast proliferation and collagen synthesis. Liver cell membranes may become immunogenic resulting in a lymphocyte-mediated cytotoxic response against the liver cells.
Clinical features
Differing patterns are seen:
· Acute alcoholic hepatitis resembles acute viral hepatitis, (malaise, anorexia, jaundice, abdominal pain and fever).
· Fatty liver is asymptomatic, it may be detected with abnormal liver function tests.
· Chronic alcohol-induced liver damage may present with signs of chronic liver damage or with complications of cirrhosis.
Microscopy
There are three main patterns of liver damage:
Alcoholic hepatitis is focal necrosis of hepatocytes, with neutrophil infiltration. Fibrosis around the central veins is present in later cases. Characteristically Mallory’s bodies composed of cytoskeletal fragments and ubiquitin, a heat shock protein that labels proteins as being damaged and targets them for breakdown. It appears as bright eosinophilic amorphous globules within hepatocytes.
Fatty change is reversible sublethal cell injury. Cells are swollen pale and vacuolated. This form of change is seen in those ingesting more than 80 g alcohol per day (6 units, 1 bottle of wine or 3 pints of beer).
Cirrhosis: Repeated damage has led to fibrosis, with damage to the normal architecture upon which function is dependent.
Complications
Acute hepatitis may rarely lead to fulminant hepatic failure. Up to 10% of patients with cirrhosis, secondary to alcohol use, develop hepatocellular carcinoma.
Investigations
Patients have deranged liver function tests especially γ GT, the MCV is also raised. Assessment of severity requires a liver biopsy, as significant liver damage can be present with a few symptoms or enzyme changes. Ultra-sound may show significant cholestasis and be mistaken for extra-hepatic obstructive jaundice.
Management
Abstinence is the best treatment. In late stages patients may be considered for liver transplant if they have proved abstinence.
Prognosis
Abstinence results in an improved prognosis, but alcohol-induced liver damage is a progressive disorder continuing to cirrhosis in many patients despite absti-nence.
· Fatty liver is reversible, with complete recovery.
· Asymptomatic patients with biopsy-proven alcoholic hepatitis who continue to drink progress to cirrhosis in 90%. However, if they abstain from drinking 90% have a full recovery.
· Patients with established cirrhosis who present with an acute episode of hepatitis have the poorest prognosis (∼60–70% 5-year survival rate).
Related Topics