Chapter: Medical Physiology: Parathyroid Hormone, Calcitonin, Calcium and Phosphate Metabolism, Vitamin D, Bone, and Teeth
Physiology of the Teeth
Physiology of the Teeth
The teeth cut, grind, and mix the food eaten. To perform these functions, the jaws have powerful muscles capable of providing an occlusive force between the front teeth of 50 to 100 pounds and for the jaw teeth, 150 to 200 pounds. Also, the upper and lower teeth are provided with projections and facets that interdigitate, so that the upper set of teeth fits with the lower. This fitting is called occlusion, and it allows even small particles of food to be caught and ground between the tooth surfaces.
Function of the Different Parts of the Teeth
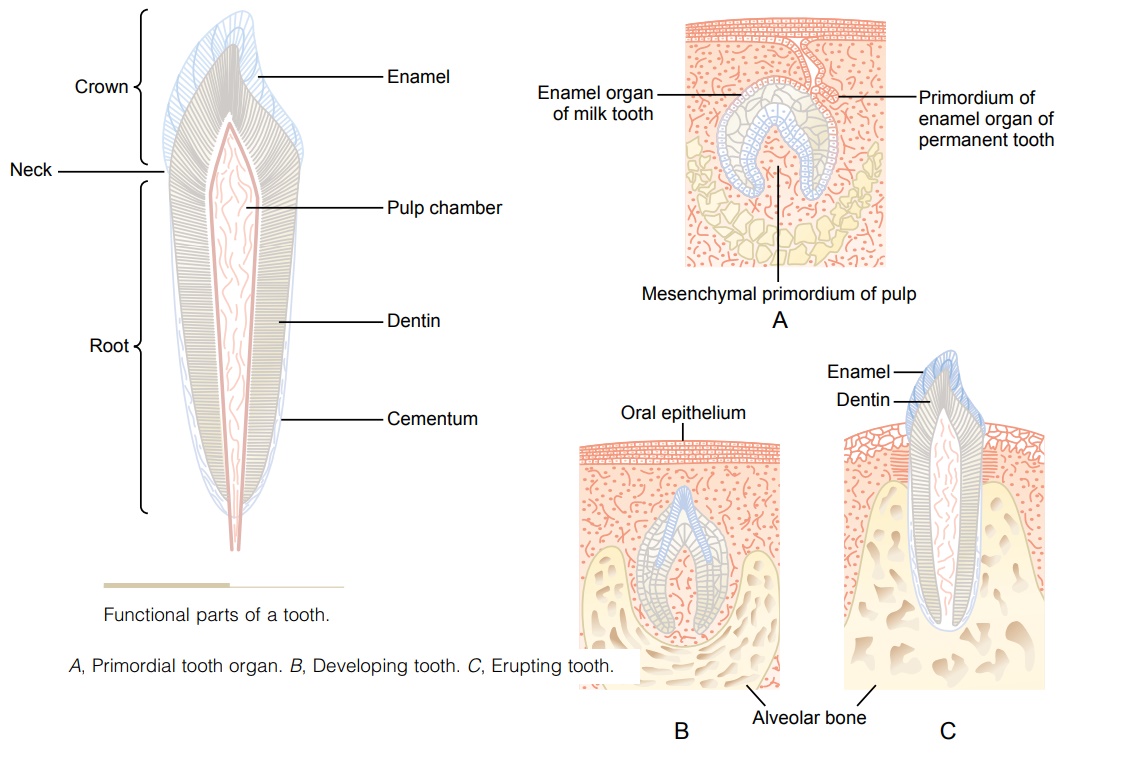
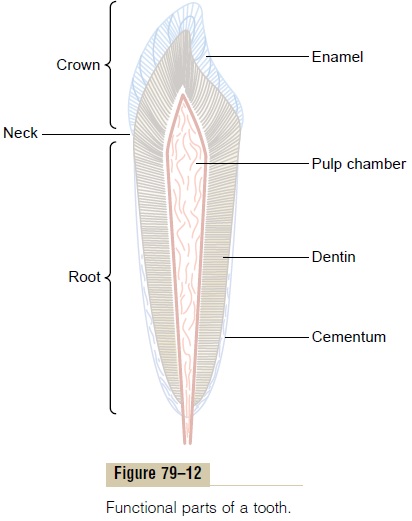
Figure 79–12 shows a sagittal section of a tooth, demonstrating its major functional parts: the enamel, dentin, cementum, and pulp. The tooth can also bedivided into the crown, which is the portion that pro-trudes out from the gum into the mouth, and the root, which is the portion within the bony socket of the jaw. The collar between the crown and the root where the tooth is surrounded by the gum is called the neck.
Enamel. The outer surface of the tooth is covered by alayer of enamel that is formed before eruption of the tooth by special epithelial cells calledameloblasts. Once the tooth has erupted, no more enamel is formed. Enamel is composed of very large and very dense crystals of hydroxyapatite with adsorbed carbonate, magnesium, sodium, potassium, and other ions imbedded in a fine meshwork of strong and almost insoluble protein fibers that are similar in phys-ical characteristics (but not chemically identical) to the keratin of hair.
The crystalline structure of the salts makes the enamel extremely hard-much harder than the dentin. Also, the special protein fiber meshwork, although constituting only about 1 per cent of the enamel mass, makes enamel resistant to acids, enzymes, and other corrosive agents because this protein is one of the most insoluble and resistant proteins known.
Dentin. The main body of the tooth is composed ofdentin, which has a strong, bony structure. Dentin is made up principally of hydroxyapatite crystals similar to those in bone but much more dense. These crystals are imbedded in a strong meshwork of collagen fibers. In other words, the principal constituents of dentin are very much the same as those of bone. The major dif-ference is its histological organization, because dentin does not contain any osteoblasts, osteocytes, osteo-clasts, or spaces for blood vessels or nerves. Instead, it is deposited and nourished by a layer of cells calledodontoblasts, which line its inner surface along the wallof the pulp cavity.
The calcium salts in dentin make it extremely resist-ant to compressional forces, and the collagen fibers make it tough and resistant to tensional forces that might result when the teeth are struck by solid objects.
Cementum. Cementum is a bony substance secretedby cells of the periodontal membrane, which lines the tooth socket. Many collagen fibers pass directly from the bone of the jaw, through the periodontal membrane, and then into the cementum. These colla-gen fibers and the cementum hold the tooth in place. When the teeth are exposed to excessive strain, the layer of cementum becomes thicker and stronger. Also, it increases in thickness and strength with age, causing the teeth to become more firmly seated in the jaws by adulthood and later.
Pulp. The pulp cavity of each tooth is filled withpulp,which is composed of connective tissue with an abun-dant supply of nerve fibers, blood vessels, and lym-phatics. The cells lining the surface of the pulp cavity are the odontoblasts, which, during the formative years of the tooth, lay down the dentin but at the same time encroach more and more on the pulp cavity, making it smaller. In later life, the dentin stops growing and the pulp cavity remains essentially constant in size. However, the odontoblasts are still viable and send projections into small dentinal tubules that penetrate all the way through the dentin; they are of importance for exchange of calcium, phosphate, and other miner-als with the dentin.
Dentition
Humans and most other mammals develop two sets of teeth during a lifetime. The first teeth are called the deciduous teeth, or milk teeth, and they number 20 inhumans. They erupt between the 7th month and the 2nd year of life, and they last until the 6th to the 13th year. After each deciduous tooth is lost, a permanent tooth replaces it, and an additional 8 to 12 molars appear posteriorly in the jaws, making the total number of permanent teeth 28 to 32, depending on whether the four wisdom teeth finally appear, which does not occur in everyone.
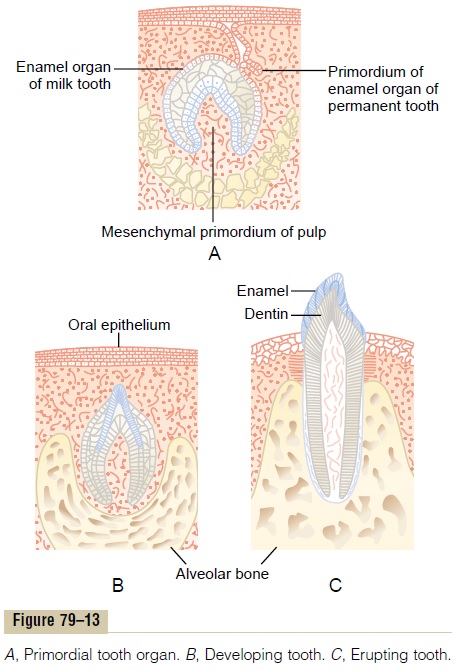
Formation of the Teeth. Figure 79–13 shows the forma-tion and eruption of teeth. Figure 79–13A shows invagination of the oral epithelium into thedentallamina; this is followed by the development of a tooth-producing organ. The epithelial cells above form ameloblasts, which form the enamel on the outside of the tooth. The epithelial cells below invaginate upward into the middle of the tooth to form the pulp cavity and the odontoblasts that secrete dentin. Thus, enamel is formed on the outside of the tooth, and dentin is formed on the inside, giving rise to an early tooth, as shown in Figure 79–13B.
Eruption of Teeth. During early childhood, the teethbegin to protrude outward from the bone through the oral epithelium into the mouth. The cause of “erup-tion” is unknown, although several theories have been offered in an attempt to explain this phenomenon. The most likely theory is that growth of the tooth root as well as of the bone underneath the tooth progressively shoves the tooth forward.
Development of the Permanent Teeth. During embry-onic life, a tooth-forming organ also develops in the deeper dental lamina for each permanent tooth that will be needed after the deciduous teeth are gone. These tooth-producing organs slowly form the perma-nent teeth throughout the first 6 to 20 years of life. When each permanent tooth becomes fully formed, it, like the deciduous tooth, pushes outward through the bone. In so doing, it erodes the root of the deciduous tooth and eventually causes it to loosen and fall out. Soon thereafter, the permanent tooth erupts to take the place of the original one.
Metabolic Factors Influence Development of the Teeth.
The rate of development and the speed of eruption of teeth can be accelerated by both thyroid and growth hormones. Also, the deposition of salts in the early-forming teeth is affected considerably by various factors of metabolism, such as the availability of calcium and phosphate in the diet, the amount of vitamin D present, and the rate of PTH secretion.When all these factors are normal, the dentin and enamel will be correspondingly healthy, but when they are defi-cient, the calcification of the teeth also may be defec-tive, so that the teeth will be abnormal throughout life.
Mineral Exchange in Teeth
The salts of teeth, like those of bone, are composed of hydroxyapatite with adsorbed carbonates and various cations bound together in a hard crystalline substance. Also, new salts are constantly being deposited while old salts are being reabsorbed from the teeth, as occurs in bone. Deposition and reabsorption occur mainly in the dentin and cementum and to a very limited extent in the enamel. In the enamel, these processes occur mostly by diffusional exchange of minerals with the saliva instead of with the fluids of the pulp cavity.
The rate of absorption and deposition of minerals in the cementum is about equal to that in the surround-ing bone of the jaw, whereas the rate of deposition and absorption of minerals in the dentin is only one third that of bone. The cementum has characteristics almost identical to those of usual bone, including the presence of osteoblasts and osteoclasts, whereas dentin does not have these characteristics, as explained earlier. This difference undoubtedly explains the different rates of mineral exchange.
In summary, continual mineral exchange occurs in the dentin and cementum of teeth, although the mech-anism of this exchange in dentin is unclear. However, enamel exhibits extremely slow mineral exchange, so that it maintains most of its original mineral comple-ment throughout life.
Dental Abnormalities
The two most common dental abnormalities are caries and malocclusion. Caries refers to erosion of the teeth, whereas malocclusion is failure of the projections of the upper and lower teeth to interdigitate properly.
Caries and the Role of Bacteria and Ingested Carbohydrates.
It is generally agreed that caries result from the action of bacteria on the teeth, the most common of which is Streptococcus mutans. The first event in the develop-ment of caries is the deposit of plaque, a film of pre-cipitated products of saliva and food, on the teeth. Large numbers of bacteria inhabit this plaque and are readily available to cause caries. These bacteria depend to a great extent on carbohydrates for their food. When carbohydrates are available, their meta-bolic systems are strongly activated and they multiply. In addition, they form acids (particularly lactic acid) and proteolytic enzymes. The acids are the major culprit in causing caries because the calcium salts of teeth are slowly dissolved in a highly acidic medium.
And once the salts have become absorbed, the remain-ing organic matrix is rapidly digested by the prote-olytic enzymes.
The enamel of the tooth is the primary barrier to the development of caries. Enamel is far more resistant to demineralization by acids than is dentin, primarily because the crystals of enamel are dense, but also because each enamel crystal is about 200 times as large in volume as each dentin crystal. Once the carious process has penetrated through the enamel to the dentin, it proceeds many times as rapidly because of the high degree of solubility of the dentin salts.
Because of the dependence of the caries bacteria on carbohydrates for their nutrition, it has frequently been taught that eating a diet high in carbohydrate content will lead to excessive development of caries. However, it is not the quantity of carbohydrate ingested but the frequency with which it is eaten that is important. If carbohydrates are eaten in many small parcels throughout the day, such as in the form of candy, the bacteria are supplied with their preferential metabolic substrate for many hours of the day, and the development of caries is greatly increased.
Role of Fluorine in Preventing Caries. Teeth formed in chil-dren who drink water that contains small amounts of fluorine develop enamel that is more resistant to caries than the enamel in children who drink water that does not contain fluorine. Fluorine does not make the enamel harder than usual, but fluorine ions replace many of the hydroxyl ions in the hydroxyapatite crys-tals, which in turn makes the enamel several times less soluble. Fluorine may also be toxic to the bacteria. Finally, when small pits do develop in the enamel, flu-orine is believed to promote deposition of calcium phosphate to “heal” the enamel surface. Regardless of the precise means by which fluorine protects the teeth, it is known that small amounts of fluorine deposited in enamel make teeth about three times as resistant to caries as teeth without fluorine.
Malocclusion. Malocclusion is usually caused by ahereditary abnormality that causes the teeth of one jaw to grow to abnormal positions. In malocclusion, the teeth do not interdigitate properly and therefore cannot perform their normal grinding or cutting action adequately. Malocclusion occasionally also results in abnormal displacement of the lower jaw in relation to the upper jaw, causing such undesirable effects as pain in the mandibular joint and deterioration of the teeth.
The orthodontist can usually correct malocclusion by applying prolonged gentle pressure against the teeth with appropriate braces. The gentle pressure causes absorption of alveolar jaw bone on the com-pressed side of the tooth and deposition of new bone on the tensional side of the tooth. In this way, the tooth gradually moves to a new position as directed by the applied pressure.
Related Topics