Chapter: Medicine and surgery: Genitourinary system
Haematuria and discoloured urine - Clinical Symptoms
Haematuria and discoloured urine
Haematuria is blood in the urine, which may be macrosopic or microscopic. Macroscopic haematuria is suggested by a reddish or pink discoloration of the urine, or may range to the passage of bright red, dark or even clotted blood. Microscopic haematuria can only be diagnosed by use of a ŌĆśdipstickŌĆÖ test, or on microscopy, as it cannot be seen by the naked eye.
Blood can come from anywhere within the urinary tract, from the glomeruli, down to the urethra. Pink tinged urine at the start of micturition, which then clears, suggests urethral inflammation/trauma or prostatic disease. Haematuria that only occurs at the end of micturition suggests disease of the trigone of the bladder.
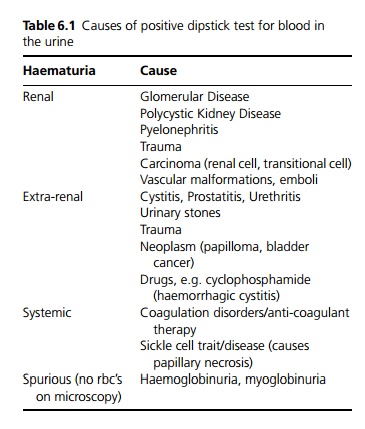
When the urine appears pink, but does not contain red blood cells on urine microscopy, this is ŌĆśspurious haematuriaŌĆÖ. If the dipstick test is positive, then this means that there is either haemoglobin or myoglobin in the urine, such as occurs in rhabdomyolysis. Certain drugs (such as rifampicin) and beetroot ingestion can make the urine appear orange, pink or red, but the dipstick test will be negative (see Table 6.1).
Dark urine should not be interpreted as ŌĆśconcentratedŌĆÖ, as this is an unreliable sign. Dark urine does occur in conjunction with pale stools in obstructive jaundice. Urine turns dark after standing for some time in porphyria. Cloudy urine has many causes, including pus (pyuria), blood (ŌĆśsmokyŌĆÖ urine) and phosphate crystals. A high concentration of phosphate in the urine is quite common, usually completely benign, and can be reduced by drinking plenty of fluids (not milk), but occasionally can signify a tendency to develop urinary stones.
Clinical features
It is important to take a history, which may suggest a cause:
Dysuria suggests cystitis. This should be treated, then urine retested to ensure the haematuria has cleared.
Renal colic, or a previous history of urinary stones. Recent upper respiratory tract infection suggests IgA
nephropathy or post-infectious glomerulonephritis.
If the patient is a female of childbearing age ensure she is not menstruating (repeat the test mid-cycle).
A drug history, including anti-coagulants such as warfarin.
Occupational history (for exposure to carcinogens).
A history or family history of polycystic kidneys, or other kidney disease.
Perform an examination including blood pressure. Urine dipstick is vital and considered part of the clinical examination.
Investigations
Transient microscopic haematuria (without proteinuria) without any other symptoms or signs is generally benign, and may be followed up clinically in young individuals.
Separate samples of urine can be collected on commencing micturition, midway through micturition and at the end of micturition (the three-glass test).
┬Ę If haematuria is greatest in the first sample the source of bleeding is likely to be the anterior urethra.
┬Ę Haematuria greatest in the third glass suggests a source in posterior urethra, bladder neck or trigone (base of the bladder).
┬Ę Haematuria that occurs equally in all glasses indicates bleeding in the bladder or upper urinary tract.
It is useful to try to differentiate between urological and nephrological causes, after initial tests such as a midstream urine for culture, urine microscopy looking for casts, FBC and U&Es, to determine which further investigations are needed and which specialist should see the patient. A raised urea and creatinine may be caused by nephrological or urological cause, such as glomerular disease or urinary obstruction (see Fig. 6.1).
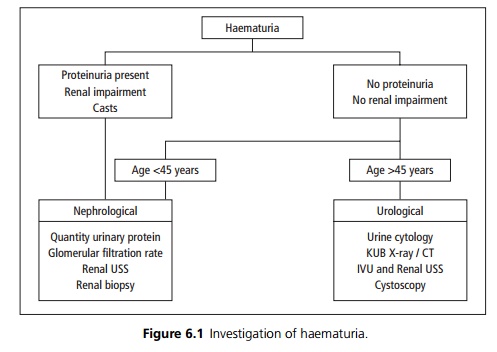
If there is proteinuria or red cell casts, glomerular disease should be suspected, and patients should be referred to a nephrologist.
In the absence of proteinuria, it is important to exclude cancer of the urinary tract and patients should be referred to a urologist.
Related Topics