Chapter: Case Study in Obstetrics and Gynaecology: Early Pregnancy
Case Study Reports: Bleeding and Pain in Early Pregnancy
BLEEDING AND PAIN IN EARLY PREGNANCY
History
A
27-year-old woman attends
the emergency department with irregular vaginal
bleeding and abdominal discomfort.
She
noticed the bleeding 2 days previously and it is dark red,
sufficient for her
to need to wear
a sanitary towel,
but not heavy.
The abdominal discomfort is suprapubic and crampy, slightly more on the right-hand side. She is systemically well
with no fever, change in appetite, nausea or vomiting.
She says that her bowel and urinary
habits are normal. Her last menstrual period commenced 45 days previously and she usually
has a slightly irregular cycle, bleeding for
3–5 days every
28–35 days. She
has never been
preg- nant. She has
been with her
regular sexual partner
for 2 years and they
generally use con- doms but there are some occasions where they do not. She had a sexual health
screen 6 months ago at the genitourinary clinic
where she was told all her swabs
were negative. She has no previous
gynaecological history and no significant previous medical problems.
Examination
The blood pressure is 128/72 mmHg
and heart rate is 82/min. The abdomen is soft and non-distended. There is
tenderness on deep palpation in the suprapubic and right iliac fossa regions,
but no rebound tenderness or guarding. Bimanual examination is not performed.
Questions
·
What is the diagnosis?
·
What are the management options in this case?
·
How
would you counsel
the woman postoperatively?
ANSWER
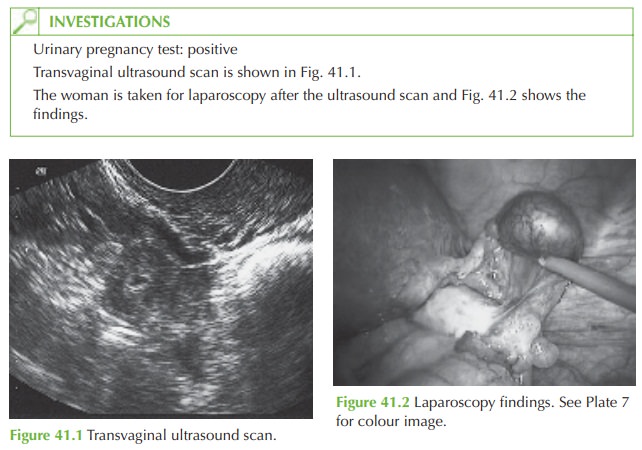
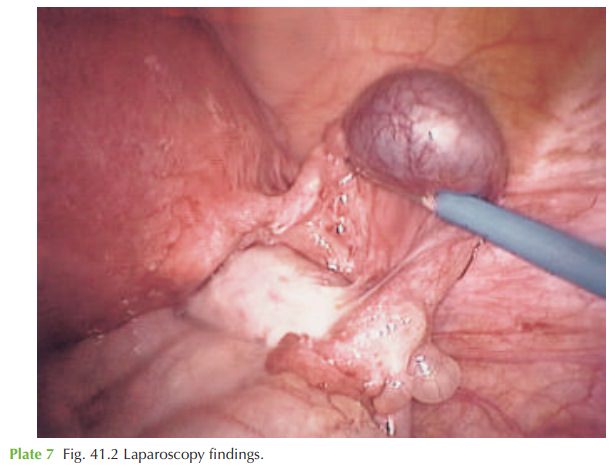
The
diagnosis is an ectopic pregnancy. This can be seen from the positive
pregnancy test, ultrasound confirming a pregnancy in the adnexa (with fetal heart beat present in this
case), and laparoscopic confirmation of a distended
right uterine tube, showing the typical
bluish bulge. There
is no evidence of blood
in the pouch
of Douglas (haemoperitoneum) to suggest rupture of the ectopic
pregnancy.
Classic symptoms of ectopic
pregnancy are amenorrhoea, iliac fossa pain and dark vaginal bleeding. Ectopic pregnancies are, however, often
diagnosed in women
with any combination of symptoms from heavy vaginal
bleeding with clots to period-type pain, to no symptoms
at all. Ectopic pregnancies occur in 1–2 per cent of pregnancies and the majority are diagnosed before
rupture but occasionally women still present
with collapse and this is a medical emergency – a woman
with collapse and a positive
pregnancy test should be initially assumed
to have a ruptured ectopic
pregnancy.
Management options
General ectopic pregnancy management
options are:
·
surgical (salpingectomy or salpingotomy)
·
medical (methotrexate injection)
·
expectant (wait and see).
In
this case, the only option
is surgical in view of the fact that a fetal heart
beat is pre- sent, rendering conservative options
both dangerous (because of risk of rupture) and unlikely to be successful. The ectopic pregnancy should be removed
laparoscopically if possible to minimize hospital
stay and postoperative pain and to reduce postoperative complications including adhesions. If the contralateral tube is healthy,
then the tube may
be removed (salpingectomy). If the
other is damaged
then salpingotomy (incision into
the tube to remove the pregnancy) should be attempted.
Related Topics