Chapter: Case Study in Obstetrics and Gynaecology: Early Pregnancy
Case Study Reports: Early Pregnancy Ultrasound
EARLY PREGNANCY ULTRASOUND
History
A
25-year-old woman is referred by the general
practitioner (GP) for early pregnancy dat- ing ultrasound scan.
She is gravida
4 para 2. Her first
positive pregnancy test
was 4 days ago and she
went to her
GP to arrange a termination of pregnancy as she feels
that she cannot cope
with another child.
She has been
taking the combined oral contraceptive pill (COCP), so pregnancy could
not be dated clinically. She has no significant gynaecological history of note except
for an episode
of chlamydia aged
18 years, for
which she and
her partner were fully
treated. As a child she had a ruptured appendix
and needed a midline
laparotomy. She has no other
relevant past medical
history.
She
has had no pain though
did note some moderate vaginal
bleeding 2 weeks
before for 3 days, which
settled spontaneously.
Examination
She
looks well with normal heart
rate and blood
pressure and a soft non-tender abdomen. Speculum examination shows
a closed cervix
with a normal discharge and no blood.
The uterus feels normal size and is anteverted and mobile. There is no
cervical excitation. There is slight tenderness in the left
adnexa but no masses are
palpable.
Questions
·
How
would you interpret this ultrasound scan result?
Answer:
Serial serum human chorionic gonadotrophin (HCG) and
progesterone is requested and the results are as follows:
Day 1: serum HCG 703 IU/L, progesterone 30 nmol/L
Day 3: serum HCG 905 IU/L,
progesterone 24 nmol/L
What is the likely
diagnosis and the
differential diagnosis, and
how would you
further investigate and manage this woman?
Answer:
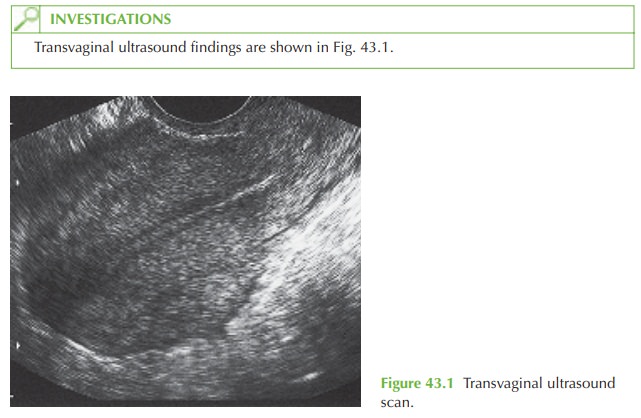
The
transvaginal ultrasound scan shows an empty uterus
and no adnexal masses. This is
therefore termed a pregnancy of unknown location
(PUL).

PUL occurs in up to 20 per cent of women in early pregnancy units and the possible
underlying diagnoses are:
·
early intrauterine pregnancy: too early to be visualized on ultrasound
·
failed pregnancy: a complete
miscarriage where the pregnancy has been completely expelled but where no previous scan is available to confirm that an intrauterine pregnancy had been present
·
ectopic pregnancy: the pregnancy is
located outside the uterine cavity but has not
been visualized at initial ultrasound examination.
Only 10 per
cent of PULs
are subsequently diagnosed as ectopic pregnancies, but all must be
investigated with serial
serum HCG to determine which
of the above three diagnoses is likely.
Serum HCG results and management
The HCG at which an intrauterine
pregnancy would normally be visualized is 1000–1500 IU/L (in most but not all cases).
A normal early
pregnancy would generally show an increase in HCG of over 66 per cent in each 48 h. The progesterone level is usually high
(>60 nmol/L) in an ongoing
pregnancy and low
(<25 nmol/L) in a failing pregnancy.
In
this case the suboptimal HCG rise and mid-range progesterone are typical (but not
diagnostic) of an ectopic pregnancy, and the woman should have a repeat ultrasound within a few days.
If an ectopic pregnancy is visualized then medical or surgical manage- ment should depend on signs and
symptoms. If a pregnancy is still not
visualized and she becomes symptomatic then laparoscopy is indicated to establish the diagnosis. If HCG
continues to rise with no apparent pregnancy
visible, then methotrexate for persistent PUL may
be considered.
Related Topics