Chapter: Case Study in Obstetrics and Gynaecology: Early Pregnancy
Case Study Reports: Pain In Early Pregnancy
PAIN IN EARLY PREGNANCY
History
A
39-year-old woman presents
with left iliac fossa pain in pregnancy. The pain is inter-
mittent and cramping. She has had difficulty sleeping because of the pain,
but has not taken any analgesia, as she is afraid that this may affect the baby. There is no vaginal bleeding.
The
woman has a long history
of secondary infertility. She had a spontaneous vaginal delivery at term 9 years ago,
and started trying
to conceive again
soon after. She
was investigated a year
ago and found
to have polycystic ovarian syndrome and
was therefore commenced on clomifene citrate.
This was her third cycle,
her last menstrual period started 45 days ago and she had a positive
pregnancy test 4 days ago.
Examination
The
woman is apyrexial with normal blood
pressure and heart
rate. She is overweight
(body mass index 32 kg/m2) and therefore examination is limited
but there is some ten- derness on deep palpation in the left
adnexa. On bimanual examination the uterus
is nor- mal size
and anteverted. There
is some left
adnexal tenderness but
no obvious masses
are palpable.
Questions
·
What can you infer about the pregnancy from this ultrasound?
·
What are the differential diagnoses for the pain?
·
How
would you further
investigate and manage this patient?
ANSWER
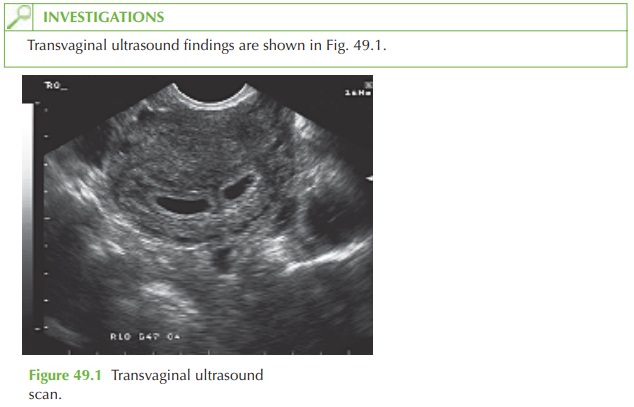
Two
distinct echolucent areas
are visible within
the endometrium. Each
has a bright tro-
phoblastic ring around confirming that these are gestation sacs. Neither sac demonstrates a definite yolk sac or fetal
pole. The findings
suggest a twin pregnancy with gestational
age of 4–5 weeks, and
this is consistent with the woman’s
last menstrual period
date. The sacs are distinct and therefore the pregnancy will definitely be dichorionic diamniotic. Zygosity cannot be determined
by this ultrasound as both dizygotic pregnancy and a monozygotic embryo
that split prior
to implantation would
give this appearance.
Differential diagnosis of pain in
this woman is:
gynaecological:
·
corpus luteal cyst
·
other non-pregnancy-related
incidental ovarian cyst
·
ovarian hyperstimulation (a rare
complication of clomifene treatment)
non-gynaecological:
·
constipation
·
gastroenteritis
·
urinary tract infection
·
renal tract calculus.
Ectopic pregnancy is ruled
out as the ultrasound confirms
an intrauterine pregnancy. Pelvic inflammatory disease is extremely uncommon
in pregnancy as is irritable
bowel syndrome.
Further investigation
The
woman should be asked about
constipation or loose
stools, urinary frequency, dysuria or loin pain.
Urinalysis for blood
(suggestive of calculus) or nitrates/leucocytes (suggest- ive of infection) should
be performed with midstream urine
sent for microscopy, culture and sensitivity if positive.
The
adnexae should normally
be examined during
the ultrasound examination. A corpus luteum is a very
common cause of pain in early pregnancy and shows a typical peripheral blood flow pattern resembling a ‘ring of fire’ on colour Doppler
examination. Corpora lutea resolve
spontaneously by 12 weeks’ gestation.
Other ovarian cysts would also be easily seen on ultrasound – most can be safely man-
aged expectantly in pregnancy unless
there is a suspicion of malignancy, torsion
or symp- toms are severe. Ovarian
hyperstimulation is also easily recognized on ultrasound scan.
If
the urinalysis is negative, there
is no suggestive history of a bowel
problem and the adnexae appear normal, then reassurance should
be given and the patient
discharged.
Related Topics