Chapter: Clinical Anesthesiology: Anesthetic Management: Airway Management
Video Laryngoscopes
VIDEO LARYNGOSCOPES
In recent years, a myriad of
laryngoscopy devices that utilize video technology have revolution-ized
management of the airway. Direct laryngos-copy with a Macintosh or Miller blade
mandates appropriate alignment of the oral, pharyngeal, and laryngeal
structures to facilitate a direct view of the glottis. Various maneuvers, such
as the “sniff-ing” position and external movement of the larynx with cricoid
pressure during direct laryngoscopy, are used to improve the view. Video- or
optically-based laryngoscopes have either a video chip (DCI system, GlideScope,
McGrath, Airway) or a lens/ mirror (Airtraq) at the tip of the intubation blade
to transmit a view of the glottis to the operator. These devices differ in the
angulation of the blade, the presence of a channel to guide the tube to the
glottis, and the single use or multiuse nature of the device.
Video or indirect laryngoscopy most
likely offers minimal advantage in patients with uncompli-cated airways. However,
use in these patients is valu-able as a training guide for learners, especially
when the trainee is performing a direct laryngoscopy with the device while the
instructor views the glot-tis on the video screen. Additionally, use in
uncom-plicated airway management patients improves familiarity with the device
for times when direct laryngoscopy is not possible.
Indirect laryngoscopes generally improve
visu-alization of laryngeal structures in difficult air-ways; however,
visualization does not always lead to successful intubation. An endotracheal
tube sty-let is recommended when video laryngoscopy is to be performed. Some
devices come with stylets designed to facilitate intubation with that
particu-lar device. Bending the stylet and endotracheal tube in a manner
similar to the bend in the curve of the blade often facilitates passage of the
endotracheal tube into the trachea. Even when the glottic opening is seen
clearly, directing the endotracheal tube into

the trachea can be difficult. Should the
tube become caught on the arytenoids, slightly pulling the blade farther out
may better permit tube passage.Indirect laryngoscopy may result in less
dis-placement of the cervical spine; however, all pre-cautions associated with
airway manipulation in a patient with a possible cervical spine fracture should
be maintained.
·
Varieties of indirect laryngoscopes include:
·
Various
Macintosh and Miller blades in pediatric and adult sizes have video capability
in the Storz DCI system. The system can also incorporate an optical intubating
stylet (Figure
19–17). The blades are similar to conventional intubation blades,
permitting direct laryngoscopy and indirect video laryngoscopy. Assistants and
instructors are able to see the view obtained by the operator and adjust their
maneuvers accordingly to facilitate intubation or to provide instruction,
respectively.
·
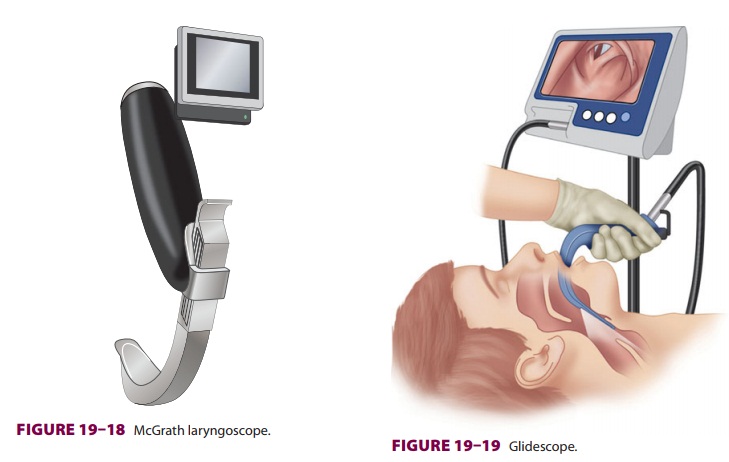
The
McGrath laryngoscope is a portable video laryngoscope with a blade length that
can be adjusted to facilitate a child of age 5 years up to an adult ( Figure
19–18). The blade can be disconnected from the handle to facilitate its
insertion in morbidly obese patients in whom the space between the upper chest
and head is reduced. The blade is inserted midline, with the laryngeal structures
viewed at a distance to enhance intubation success.

·
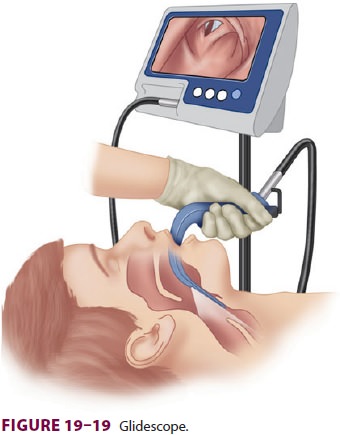
The
GlideScope comes with disposable adult-and pediatric-sized blades (Figure 19–19).
The blade is inserted midline and advanced until glottic structures are
identified. The GlideScope has a 60°
angle, preventing direct laryngoscopy and necessitating the use of stylet that
is similar in shape to the blade.
·
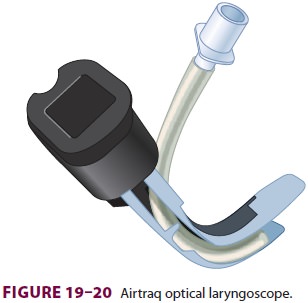
Airtraq
is a single-use optical laryngoscope available in pediatric and adult sizes (Figure 19–20).
The device has a channel to guide the endotracheal tube to the glottis. This
device is inserted midline. Success is more likely when the device is not
positioned too close to the glottis.
·
Video
intubating stylets have a video capability and light source. The stylet is
introduced, and the glottis identified. Intubation with a video stylet may
result in less cervical spine movement than with other techniques.
Flexible Fiberoptic Bronchoscopes
In some situations—for example, patients with unstable cervical spines, poor range of motion of the temporomandibular joint, or certain congenital or acquired upper airway anomalies—laryngoscopy with direct or indirect laryngoscopes may be unde-sirable or impossible. A flexible FOB allows indi-rect visualization of the larynx in such cases or in any situation in which awake intubation is planned (Figure 19–21). Bronchoscopes are constructed of coated glass fibers that transmit light and images by internal reflection (ie, a light beam becomes trapped
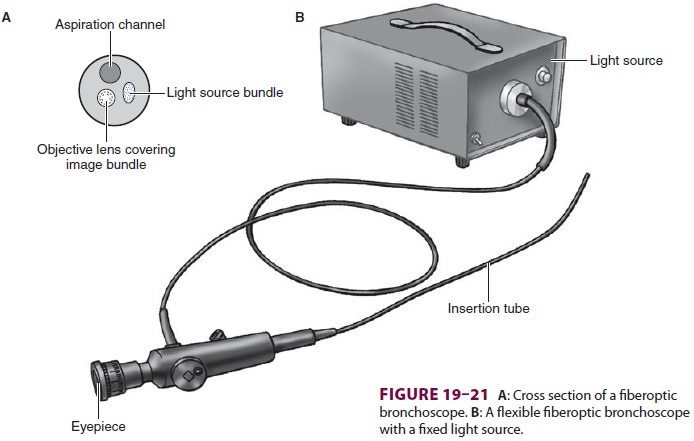
within a fiber and exits unchanged at
the opposite end). The insertion tube contains two bundles of fibers, each
consisting of 10,000 to 15,000 fibers. One bundle transmits light from the
light source (light source or incoherent bundle), which is either external to
the device or contained within the han-dle (Figure 19–21B), whereas the other
provides a high-resolution image (image or coherent bundle). Directional
manipulation of the insertion tube is accomplished with angulation wires.
Aspiration channels allow suctioning of secretions, insuffla-tion of oxygen, or
instillation of local anesthetic. Aspiration channels can be difficult to
clean, and, if not properly cleaned and sterilized after each use, may provide
a nidus for infection.
Related Topics