Chapter: Clinical Anesthesiology: Anesthetic Management: Airway Management
Airway Management Equipment
EQUIPMENT
Preparation is mandatory for all airway
manage-ment scenarios. The following equipment is rou-tinely needed in airway
management situations:
·
An
oxygen source
·
BMV
capability
·
Laryngoscopes
(direct and video)
·
Several
endotracheal tubes of different sizes
·
Other
(not endotracheal tube) airway devices (eg, oral, nasal airways)
·
Suction
·
Oximetry
and CO2 detection
·
Stethoscope
·
Tape
·
Blood
pressure and electrocardiography (ECG) monitors
·
Intravenous
access
Oral & Nasal Airways
Loss of upper airway muscle tone (eg,
weakness of the genioglossus muscle) in anesthetized patients allows the tongue
and epiglottis to fall back against the pos-terior wall of the pharynx.
Repositioning the head or a jaw thrust is the preferred technique for open-ing
the airway. To maintain the opening, an artificial airway can be inserted
through the mouth or nose to maintain an air passage between the tongue and the
posterior pharyngeal wall ( Figure 19–6). Awake or lightly anesthetized
patients with intact laryngeal reflexes may cough or even develop laryngospasm
during airway insertion. Placement of an oral air-way is sometimes facilitated
by suppressing airway reflexes, and, in addition, sometimes by depressing the
tongue with a tongue blade. Adult oral airways typically come in small (80 mm
[Guedel No. 3]), medium (90 mm [Guedel No. 4]), and large (100 mm [Guedel No.
5]) sizes.
The length of a nasal airway can be
estimated as the distance from the nares to the meatus of the ear and should be
approximately 2–4 cm longer than oral airways. Because of the risk of
epistaxis, nasal airways are less desirable in anticoagulated or
thrombocytopenic patients. Also, nasal air-ways (and nasogastric tubes) should
be used with caution in patients with basilar skull fractures, where there has
been a case report of a nasogastric tube entering the cranial vault. All tubes
inserted through the nose (eg, nasal airways, nasogastric
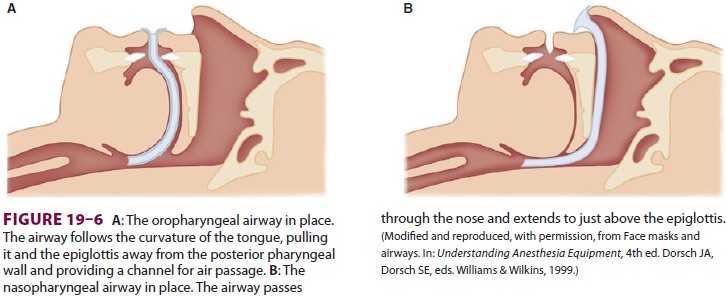
catheters, nasotracheal tubes) should be
lubricated before being advanced along the floor of the nasal passage.
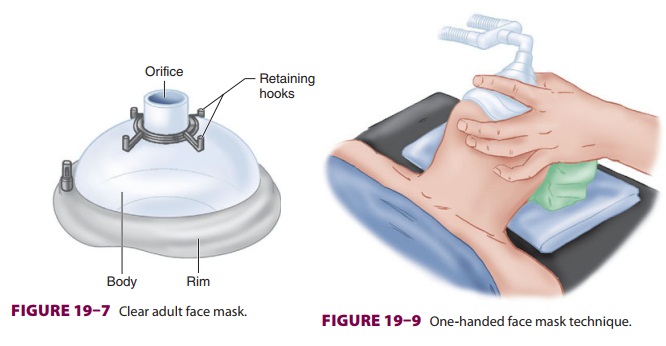
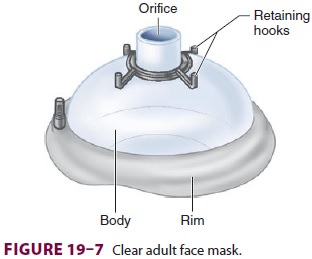
Face Mask Design & Technique
The use of a face mask can facilitate
the delivery of oxygen or an anesthetic gas from a breathing sys-tem to a
patient by creating an airtight seal with the patient’s face (Figure 19–7).
The rim of the mask is contoured and conforms to a variety of facial features.
The mask’s 22-mm orifice attaches to the breathing circuit of the anesthesia
machine through a right-angle connector. Several mask designs are available.
Transparent masks allow observation of exhaled humidified gas and imme-diate
recognition of vomitus. Retaining hooks surrounding the orifice can be attached
to a head strap so that the mask does not have to be continu-ally held in place.
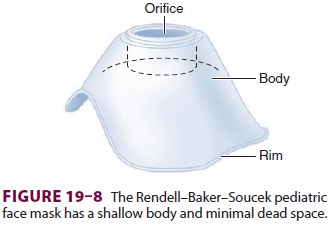
Some pediatric masks are spe-cially designed to minimize apparatus dead space (Figure 19–8).
Effective mask ventilation requires both
a gastight mask fit and a patent airway. Improper face mask technique can
result in continued deflation of the anesthesia reservoir bag when the
adjustable pressure-limiting valve is closed, usually indicating a substantial
leak around the mask. In contrast, the generation of high breathing circuit
pressures with minimal chest movement and breath sounds implies an obstructed
airway or obstructed tubing.
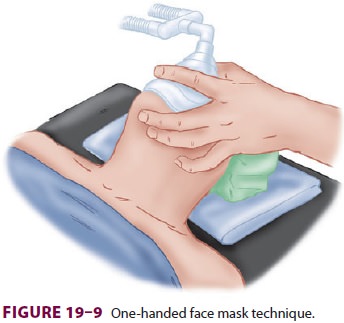
If the mask is held with the left hand,
the right hand can be used to generate positive-pressure ven-tilation by
squeezing the breathing bag. The mask is held against the face by downward
pressure on the mask body exerted by the left thumb and index fin-ger (Figure 19–9).
The middle and ring finger grasp the mandible to facilitate extension of the
atlanto-occipital joint. This is a maneuver that is easier to teach than to
describe. Finger pressure should be placed on the bony mandible and not on the
soft tis-sues supporting the base of the tongue, which may obstruct the airway.
The little finger is placed under the angle of the jaw and used to thrust the
jaw ante-riorly, the most important maneuver to allow venti-lation to the
patient.

In difficult situations, two hands may
be needed to provide adequate jaw thrust and to create a mask seal. Therefore,
an assistant may be needed to squeeze the bag, or the machine’s ventilator can
be used. In such cases, the thumbs hold the mask down, and the fingertips or
knuckles displace the jaw for-ward (Figure 19–10). Obstruction during expira-tion
may be due to excessive downward pressure from the mask or from a ball-valve
effect of the jaw thrust. The former can be relieved by decreasing the pressure
on the mask, and the latter by releasing the jaw thrust during this phase of
the respiratory cycle. It is often difficult to form an adequate mask fit with
the cheeks of edentulous patients. Positive-pressure ventilation using a mask
should normally be limited to 20 cm of H2O
to avoid stomach inflation.
Most patients’ airways can be maintained
with a face mask and an oral or nasal airway. Mask ventila-tion for long
periods may result in pressure injury to branches of the trigeminal or facial
nerves. Because of the absence of positive airway pressures dur-ing spontaneous
ventilation, only minimal down-ward force on the face mask is required to
create an adequate seal. If the face mask and mask straps are used for extended
periods, the position should be regularly changed to prevent injury. Care
should be used to avoid mask or finger contact with the eye, and the eyes should
be taped shut to minimize the risk of corneal abrasions.
Related Topics