Chapter: Clinical Anesthesiology: Anesthetic Management: Airway Management
Surgical Airway Techniques
SURGICAL AIRWAY TECHNIQUES
“Invasive” airways are required when the
“can’t intu-bate, can’t ventilate” scenario presents and may be performed in
anticipation of such circumstances in selected patients. The options include:
surgical cricothyrotomy, catheter or needle cricothyrotomy, transtracheal
catheter with jet ventilation, and retro-grade intubation.
Surgical cricothyrotomy refers to
surgical incision of the CTM and placement of a breath-ing tube. More recently,
several needle/dilator cricothyrotomy kits have become available. Unlike
surgical cricothyrotomy, where a horizontal inci-sion is made across the CTM,
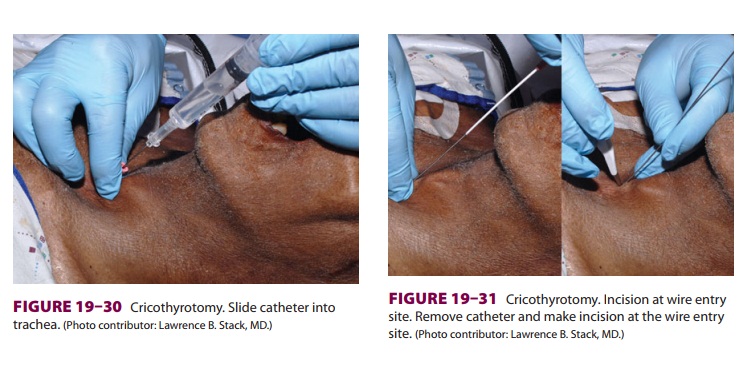
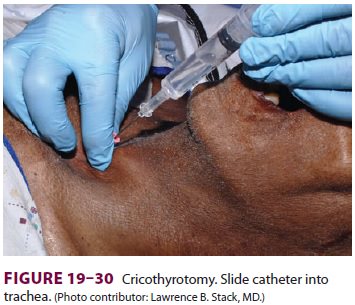
these kits utilize the Seldinger catheter/wire/dilator technique. A catheter
attached to a syringe is inserted across the CTM (Figure 19–30). When air is
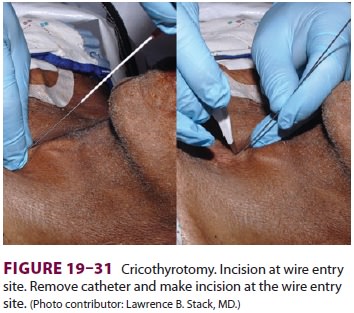
aspirated, a guidewire is passed through the catheter into the trachea ( Figure 19–31).
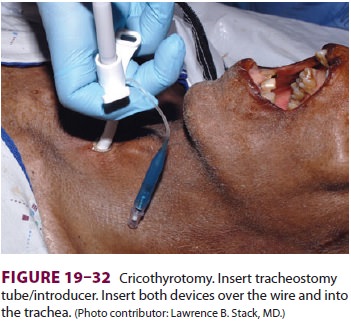
A dilator is then passed over the guidewire, and a breathing tube placed (Figure 19–32).
Catheter-based salvage procedures can
also be performed. A 16- or 14-gauge intravenous cannula is attached to a
syringe and passed through the CTM toward the carina. Air is aspirated. If a
jet ventila-tion system is available, it can be attached. The cath-eter MUST be
secured, otherwise the jet pressure will push the catheter out of the airway,
leading to potentially disastrous subcutaneous emphysema. Short (1 s) bursts of
oxygen ventilate the patient. Sufficient outflow of expired air must be assured
to avoid barotrauma. Patients ventilated in this manner may develop
subcutaneous or mediastinal emphysema and may become hypercapneic despite
adequate oxygenation. Transtracheal jet ventilation will usually require
conversion to a surgical airway or tracheal intubation.
Should a jet ventilation system not be available, a 3-mL syringe can be attached to the catheter and the syringe plunger removed. A 7.0-mm internal diameter TT connector can be inserted into the syringe and attached to a breathing circuit or an ambu bag. As with the jet ventilation system, ade-quate exhalation must occur to avoid barotraumas.
Retrograde intubation is another
approach to secure an airway. A wire is passed via a catheter placed in the
CTM. The wire is angulated cephalad and emerges either through the mouth or
nose. The distal end of the wire is secured with a clamp to prevent it from
passing through the CTM. The wire can then be threaded into an FOB with a
loaded endotracheal tube to facilitate and confirm placement. Conversely, a
small endotracheal tube can be guided by the wire into the trachea. Once
placed, the wire is removed. Alternatively, an epidural catheter can be placed
via an epidural needle in the CTM. After the distal end is retrieved from the
mouth, an endotracheal tube may be passed over the catheter into the trachea.
Related Topics