Chapter: Essentials of Psychiatry: Delirium and Dementia
Vascular Dementia
Vascular Dementia
Vascular dementia usually results from multiple CVAs or one significant CVA. It is generally considered the second most com-mon cause of dementia after Alzheimer’s disease, accounting for about 10% of all cases. Men are twice as likely as women to be diagnosed with this condition. Vascular dementia is character-ized by a stepwise progression of cognitive deterioration with ac-companying lateralizing signs. It is always associated with evi-dence of systemic hypertension and usually involves renal and cardiac abnormalities. Risk factors for the development of a vas-cular dementia include those generally associated with obstruc-tive coronary artery disease, including obesity, hypercholestero-lemia, smoking, hypertension, stress and lack of exercise. The actual incidence of vascular dementia has decreased somewhat with better standards of care, improved diagnostic techniques and lifestyle changes.
Clinical Features
Vascular dementia is characterized by the early
appearance of local-izing neurological signs. Spasticity, hemiparesis, ataxia
and pseu-dobulbar palsy are common. Pseudobulbar palsy is associated with
injury to the frontal lobes and results in impairment of the corticob-ulbar
tracts. It is characterized by extreme emotional lability, abnor-mal speech
cadence, dysphagia, hyperactive jaw jerk, hyperactive deep tendon reflexes and
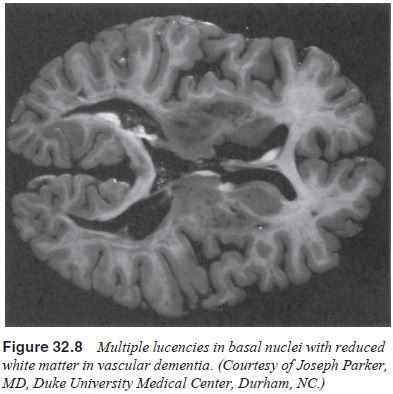
Babinski’s reflex. CT, MRI and gross spec-imens show cerebral atrophy and
infarctions, with the radiological procedures showing multiple lucencies and
the gross specimens revealing distinct white matter lesions (Figure 32.8). The
EEG is ab-normal but nonspecific, and positron emission tomography reveals
hypometabolic areas. Vascular dementia is differentiated from AD on the basis
of its mode of progression, early appearance of neuro-logical signs, and
radiographical evidence of cerebral ischemia.
Treatment
Primary prevention and secondary prevention are
important in the treatment of cerebrovascular disorders. Lifestyle changes are
effective in arresting the progress of the disease; however, no known
pharmacological treatment can reverse the effects of a completed stroke. Such
interventions as anticoagulants for fre-quent transient ischemic attacks after
a hemorrhagic lesion have been investigated but excluded; aspirin for
decreasing platelet ag-gregation, and surgical removal of obstructing plaques
probably do not reverse the mental state. Depression occurs in 50 to 60% of
patients with CVAs and responds to traditional antidepressants. Tricyclic
antidepressants, such as amitriptyline, in less than anti-depressant doses,
improve both CVA depression and pseudobul-bar palsy. Physical rehabilitation is
essential and often results in an improvement in mood and outlook.
Related Topics