Chapter: Basic Radiology : Radiology of the Urinary Tract
Ultrasonography - Radiology of the Urinary Tract: Techniques and Normal Anatomy
Ultrasonography
Ultrasound is a useful technique
for evaluation of the urinary tract, with its principal advantages including
wide availabil-ity, no need for intravenous contrast material, and lack of
ionizing radiation. The kidneys are generally well seen by a posterior or
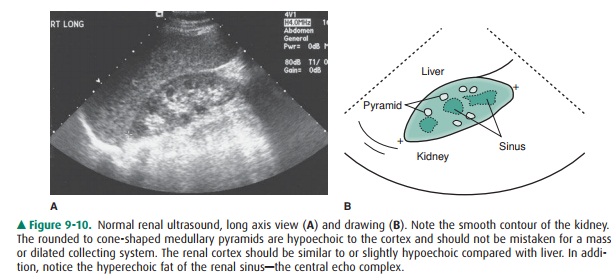
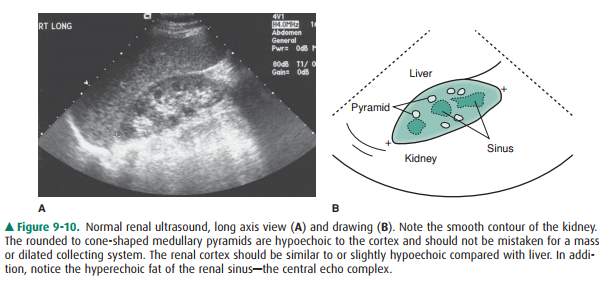
lateral approach in all but the largest of patients (Figure 9-10). The renal
medulla is hypoechoic (darker) rela-tive to renal cortex and can be identified
in some adults as cone-shaped central structures. In some patients, this
corti-comedullary distinction is not visible and should not be con-sidered
pathologic. The renal cortex is isoechoic or slightly hypoechoic compared with
the echogenicity of the adjacent liver. Renal echogenicity exceeding that of
the liver is abnor-mal and requires explanation. Most commonly, hyperechoic
kidneys are the result of medical renal disease, such as end-stage hypertensive
glomerulosclerosis. In addition to echogenicity and as with CT evaluation, the
kidneys should be assessed for size, location, and symmetry. Scarring and
masses can be evaluated. US assessment is often specific in identifying sim-ple
or mildly complicated cysts and differentiating these lesions from a solid
mass. Solid masses, however, remain nonspecific and generally require further
evaluation. There are normal variants that can mimic mass lesions, including
dromedary humps, as well as central prominences of normal renal tissue
interposed between lobes referred to as persistent columns of Bertin.
Additionally, the parenchyma near the renal hila may appear prominent as well,
occasionally mim-icking a mass. Each of these variants may be distinguished by
its normal echogenicity, lack of mass effect, and characteris-tic location.
Occasionally, additional imaging with CT or MR may be required in equivocal
masses. The renal sinus is the area engulfed by the kidney medially, harboring
the renal pelvis, arteries, veins, nerves, and lymphatics that enter and exit
the kidney, all contained within a variable amount of fat. Fat is typically
brightly echogenic on ultrasound, and fat within the renal sinus dominates the
ultrasonographic appear-ance, creating what is known as the “central echo
complex.” The size of the central echo complex is variable, often more
prominent in the elderly and minimal in the child. Absence of the central echo
complex may suggest a mass such as a urothelial carcinoma replacing the normal
fat. Alternatively, the complex may be very prominent in the benign condition
of renal sinus lipomatosis. Calcifications often have a typical appearance on
ultrasound, being brightly echogenic and re-sulting in shadowing posteriorly as
the sound waves are at-tenuated. Renal stones or calcifications may be detected
within the renal parenchyma or in the intrarenal collecting system. The
echogenicity of the normal renal sinus, however, may be problematic by
obscuring or mimicking small stones. Ultrasound is also excellent for detecting
hydronephrosis, with the distended collecting system easily recognized within
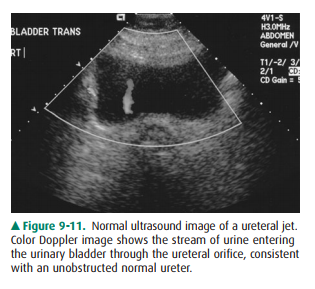
the central echo complex. The ureters are not normally seen on ultrasound
because of obscuring overlying tissue and their small size. Evidence of their
patency may be verified by Doppler detection of urine rapidly entering the
bladder from the distal ureters that is, distal ureteral jets (Figure 9-11).
The bladder is seen as a rounded or oval anechoic (fluid) structure in the
pelvis. The bladder may demonstrate mass lesions, such as transitional-cell
carcinoma, or stones. The urethra is not typically seen by ultrasound, although
urethral diverticula may occasionally be demonstrated.
Related Topics