Chapter: Basic Radiology : Radiology of the Urinary Tract
Exercise: Stone Disease
EXERCISE 9-3.
STONE DISEASE
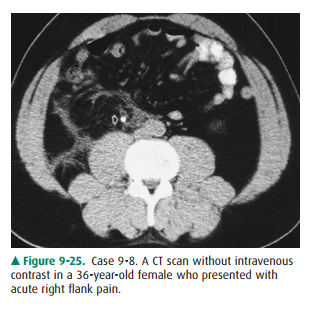
9-8. What is the most likely diagnosis for the patient in Case 9-8 (Figure 9-25)?
A.
Acute appendicitis
B.
Right ureteral calculus
C.
Ruptured aortic aneurysm
D.
Pelvic phlebolith
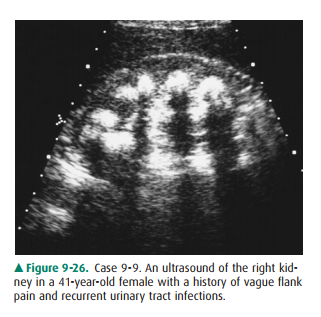
9-9. What is the most
likely diagnosis for the patient in Case 9-9 (Figure 9-26)?
A.
Medullary nephrocalcinosis
B.
Cortical nephrocalcinosis
C.
Renal tuberculosis
D.
Emphysematous pyelonephritis
Radiographic Findings
Case 9-8 (Figure 9-25) is a CT
scan of the abdomen obtained without intravenous contrast. Stranding in the fat
planes can be seen on the right in the retroperitoneum. Stranding within the
fat planes on a CT is a nonspecific finding resulting from many conditions. In
general, the stranding can be related to inflammation such as recent surgery,
infection, or abnormal fluid collections such as blood or urine. Thus, the
stranding seen in this case could result from any of the three listed pos-sible
answers. However, within the right ureter is a high-density rounded structure
(arrow) consistent with a ureteral calculus (B is the correct answer to
Question 9-8). Two main parame ters that should be noted are the size and
location of a stone, as these two factors are directly related to the
likelihood of stone passage. Additionally, once the diagnosis of a ureteral
stone is made, the radiologist must continue to evaluate the remainder of the
scan, because additional abnormalities may also exist.
In Case 9-9, a renal ultrasound (Figure 9-26) demon-strates rounded highly echogenic areas throughout the central parenchyma of the kidney. Several important additional obser-vations include strong uniform shadowing posteriorly from the echogenic areas consistent with sound attenuation and suggesting calcification. Although attenuation of the ultra-sound beam occurs with air, such as might occur with emphy-sematous pyelonephritis, the shadowing in those cases is often “dirty” in appearance, being somewhat inhomogeneous (D is incorrect). Also, the calcifications are located in the medullary area of the kidney, unlike the cortical location of cortical nephrocalcinosis (A is correct answer to Question 9-9).
Discussion
Suspected stone disease is a
common indication for urinary tract imaging. Calcifications occurring in the
kidney can be dystrophic, related to abnormal tissue such as within tumors,
cysts, or infection. This type of calcification is to be distin-guished from
nephrocalcinosis and nephrolithiasis. Nephro-calcinosis refers to the
development of calcification within the renal parenchyma, generally unrelated
to an underlying renal pathology. Furthermore, nephrocalcinosis should be
distinguished from nephrolithiasis, in which there are stones within the
collecting system. Note that nephrocalcinosis and nephrolithiasis may coexist.
Nephrocalcinosis is additionally
subdivided into two cat-egories depending on location. That which occurs in the
renal cortex is termed cortical nephrocalcinosis, and that within the medulla
is called medullary nephrocalcinosis. Cortical nephrocalcinosis is less common
and occurs most frequently in the setting of chronic glomerulonephritis or
acute cortical necrosis. Acute cortical necrosis most often oc-curs in the
setting of hypotensive shock or toxic ingestion. Cortical nephrocalcinosis may
be detected on plain radi-ographs or cross-sectional imaging modalities such as
CT or US. The diagnosis is usually made by demonstrating thin lin-ear bands of
calcification at the extreme periphery of the kid-ney that may extend into the
columns of Bertin but should not involve the renal medulla. Medullary
nephrocalcinosis is more frequently observed than cortical disease and is most
often due to hypercalcemic states such as hyperparathy-roidism, renal tubular
acidosis, or medullary sponge kidney. On plain films and CT studies, medullary
nephrocalcinosis appears as speckled or dense calcifications within the renal
medulla, sparing the cortex. In medullary sponge kidney, an anatomic condition
of abnormally dilated collecting tubules, the condition may be unilateral or
even focal, although medullary nephrocalcinosis from other causes is typically
bi-lateral and diffuse. On ultrasound, shadowing echogenic foci are noted
within the renal medulla.
Nephrolithiasis (better known as
“kidney stones”) is much more common than nephrocalcinosis. In fact, urinary
tract calculi occur in as many as 12% of the population of the United States.
Although there are clearly definable causes in some cases (hereditary
conditions, metabolic diseases such as gout, certain urinary tract infections,
and predisposing anatomic conditions), the vast majority of patients have
idiopathic stone disease. Many small stones that are located within the
intrarenal collecting system are asymptomatic; however, stones that pass into
the ureter (ureterolithiasis) may obstruct the urinary tract and result in
excruciating pain. Additionally, stones may cause hematuria or be a nidus for
recurrent infection. Conventional radiographs have long been used to evaluate
stone disease; in fact, the first descrip-tion of urinary calculi was in April
1896, only a few months after the discovery of the x-ray by Roentgen. Stones
appear as calcific densities on x-rays overlying the urinary tract (Figure
9-27). Urinary tract calculi are variably opaque and visible depending on their
size, composition, and location. The ac-curacy of conventional radiographs for
detecting stones has long been overestimated. Perhaps only 50% of stones are
identified prospectively, and one can never be certain that an individual
calcification on an isolated plain radiograph is within the urinary tract or
simply overlies it. Confusing calci-fications are many, including phleboliths,
arterial calcifica-tions, calcified lymph nodes, and other calcified masses.
Stones on ultrasound appear as brightly echogenic structures and often with
posterior shadowing. However, not all stones shadow, and as there are many
small noncalcific echogenicfoci (vessels, fat) normally within the kidney, the
accuracy for detecting renal calculi is only moderate with ultrasound.
Additionally, ultrasound suffers from its ability to visualize only the most
proximal and distal ureters and must rely on nonspecific indirect signs such as
hydronephrosis and absent ureteral jets to suggest ureteral stones and
obstruction. CT is now the imaging examination of choice for evaluation of
renal stone disease. Virtually all urinary tract stones are dense on CT and
show up as bright foci. Even stones as small as 1 mm are visible with modern
scanners. Additionally, the en-tire urinary tract can be visualized on CT
without overlap-ping or obscuring structures. In patients who present acutely
with flank pain and are suspected of having ureteral stones, CT has become the
study of choice. The diagnosis is con-firmed by directly identifying a stone
within the ureter. Sec-ondary findings of obstructing may also be identified on
CT, helping to confirm the diagnosis. Renal enlargement, perinephric stranding,
and dilation of the ureter and in-trarenal collecting system are frequently
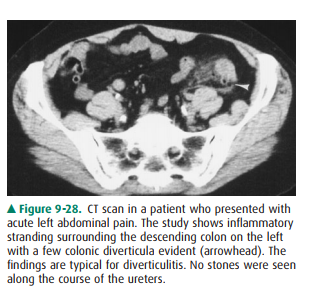
present in ureteral obstruction. One major additional advantage to CT is the
ability to identify alternative explanations for the cause of a patient’s acute
flank pain. In fact, as many as one-third of all patients originally felt to
have ureteral stones are shown byCT to have an alternative diagnosis (Figure
9-28). At this point, MRI performs little role in the evaluation of stone
disease.

In pregnant patients with
suspected obstructing calculi, CT is not contraindicated. By using a low-dose
CT technique with lowered tube current and increased pitch, fetal dose can be
lowered to as little as 3 mGy. This is well below the thresh-old for fetal
anomalies of 50 mGy, and below the threshold for increased risk of childhood
malignancy of 10 mGy. A sim-ilar technique can also be used in other situations
where low dose is desired, such as in patients who have multiple scansfor
recurrent calculi. It should be remembered that the lowest exposure achievable
should always be pursued, and these studies should only be used in situations
where they will af-fect clinical decision making.
Bladder stones may occur
secondary to transport from the ureter or arise de novo. Most cases of bladder
stones are secondary to urinary stasis such as occurs with bladder outlet
obstruction from neurogenic bladders or prostatic enlarge-ment. The diagnosis
of bladder stones is similar to those in the upper urinary tract. Finally,
urethral stones occur, and in males the vast majority are present as a result
of passage from the bladder or above. In women, urethral stones are most
fre-quently the result of urethral diverticula, which result in uri-nary stasis
and stone formation.
Related Topics