Chapter: Clinical Dermatology: Skin tumours
Tumours of the dermis: Haemangiomas
Haemangiomas
Capillary cavernous haemangioma (strawberry naevus)
Strawberry
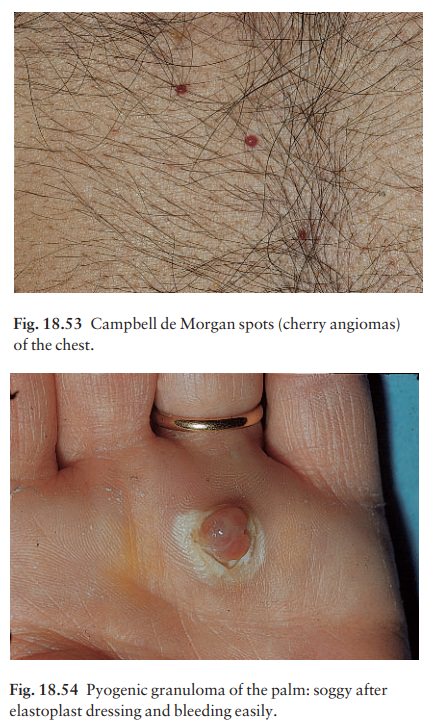
naevi appear within a few weeks of birth, and grow for a few months, forming a
raised com-pressible swelling with a bright red surface (Fig. 18.51).
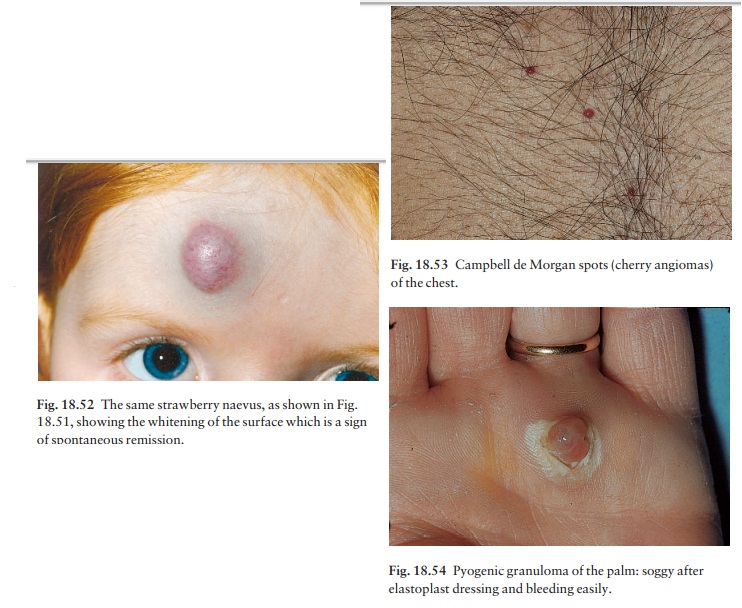
Spontaneous regression then follows; the surface whitens centrally (Fig. 18.52)
and regression is com-plete by the age of 5 years in 50% of children and in 90%
by the age of 9, leaving only an area of slight atrophy. Bleeding may follow
trauma, and ulceration is common in the napkin (diaper) area.
Observation and encouragement is the management of choice for the great majority. Serial photographs of the way they clear up in other children help parents to accept this. Firm pressure may be needed to stop bleeding. If lesions interfere with feeding, or with vision, or if giant lesions sequestrate platelets (the KasabachÔÇôMerritt syndrome), high doses of systemic steroids should be considered; they are most success-ful in the proliferative phase. Prednisolone (2ÔÇô4 mg/ kg/day) is given as a single dose in the morning and the dosage tapered to zero after 1 month. Ophthalmolo-gical help should be sought for all growing periocular haemangiomas; intralesional steroids have proved ef-fective. Sometimes pulsed tuneable dye lasers are used for treating large lesions in infancy. Rarely, plastic surgery is necessary for a few large and unsightly haemangiomas that fail to improve spontaneously or to regress with the above measures.
Campbell de Morgan spots (cherry angiomas)
These
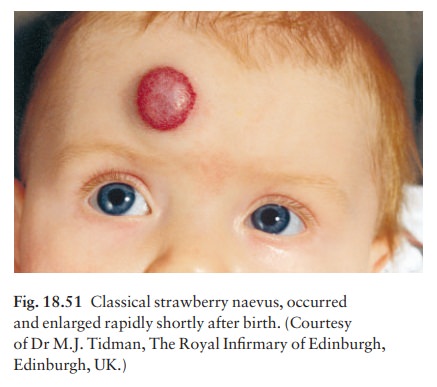
benign angiomas are common on the trunks of the middle-aged and elderly. They
are small bright red papules and of no consequence (Fig. 18.53).
Related Topics