Chapter: Clinical Dermatology: Skin tumours
Other benign dermal tumours
Other
benign dermal tumours
Dermatofibromas (histiocytomas)
These
benign tumours are firm discrete usually solit-ary dermal nodules (Fig. 18.55),
often on the extrem

The lesions have an ŌĆśicebergŌĆÖ effect in that they feel larger
than they look. The over-lying epidermis is often lightly pigmented and dimples
when the nodule is squeezed. Some lesions seem to follow minor trauma or an
insect bite. Histologically, the proliferating fibroblasts merge into the
sparsely cellular dermis at the margins. A straightforward lesion may be left
alone but, if there is any diagnostic doubt, it should be excised.
Neurofibromas
Although
solitary tumours occur occasionally, multiple neurofibromas are most common and
are usually seen as part of the inherited condition of neurofibromat-osis.
Neuroma
This rare benign tumour is usually solitary. It may appear spontaneously but is seen most often as a result of nerve injury at the site of trauma or a surgical wound. There is nothing specific about the appear-ance of the skin-coloured dermal nodule but the tumour is frequently painful, even with gentle pressure. ENGLAND is a useful acronym for painful tumours (Eccrine spiradenoma, Neuroma, Glomus tumour,
Leiomyoma, Angiolipoma, Neurofibroma (rarely) and Dermatofibroma
(rarely) ).
Keloid
This
is an overgrowth of dense fibrous tissue in the skin, arising in response to
trauma, however trivial. The tendency to develop keloids is genetically
inher-ited. Keloids are common in Negroids and may be familial. Keloid
formation is encouraged by infection, foreign material and by wounds (including
surgical ones) especially those not lying along the lines of least tension or
the skin creases. Even in Caucasoids, keloids are seen often enough on the
presternal area, the neck, upper back and deltoid region of young adults to
make doctors think twice before removing benign lesions there. Silicone
sheeting and intrale-sional steroid injections are helpful but treatment should
be given early, preferably for developing lesions.
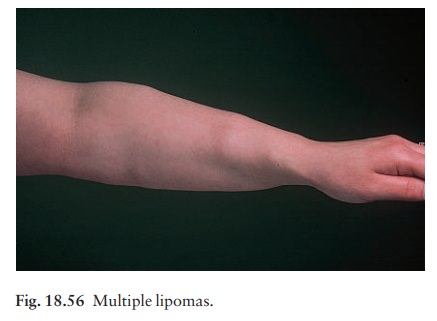
Lipomas
Lipomas are common benign tumours of mature fat cells in the subcutaneous tissue. There may be one or many (Fig. 18.56) and lipomas are rarely a familial trait. They are most common on the proximal parts of the limbs but can occur at any site. They have an irregular lobular shape and a characteristic soft rub-bery consistency. They are rarely painful. They need to be removed only if there is doubt about the dia-gnosis or if they are painful or unsightly.
Mastocytosis (urticaria pigmentosa)
This
term describes the various conditions in which the skin, and occasionally other
tissues, contains an excess of mast cells. All types are characterized by a
tendency for the skin to wheal after being rubbed. The main types are as
follow.
ŌĆó
Mastocytoma. Usually presents as a solitary
pink orbrown itchy papule which wheals on rubbing. There are no systemic
features.
ŌĆó
Juvenile mastocytosis. This is
the most commontype. Numerous pink or brown papules develop over the trunk and
limbs (Fig. 18.57). There is no systemic involvement, and the condition is
often mistaken for multiple melanocytic naevi.

ŌĆó
Diffuse cutaneous mastocytosis. This is
rare and seenmostly in infants, being characterized by persistent dermographic
wheals that appear after minor friction. The skin is diffusely infiltrated with
mast cells, pro-ducing a thickened appearance like pigskin. The bone marrow,
liver and spleen may be involved. Flushing is common. Death from massive
histamine release is a real risk. Spontaneous improvement usually occurs.
Adult
type. Pink or pink-brown telangiectatic mac-ules appear in early
adult life and can spread to cover the whole body. The liver, spleen and bone
are involved in up to 20% of cases but systemic features such as headaches,
flushing and palpitations are unusual.
Related Topics