Chapter: Clinical Dermatology: Skin tumours
Squamous cell carcinoma

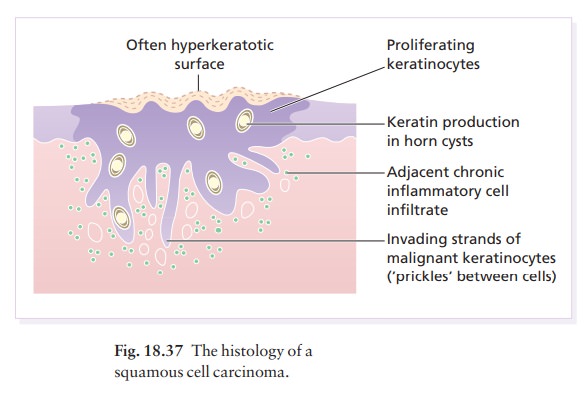
Squamous cell carcinoma
This
is a common tumour in which malignant ker-atinocytes show a variable capacity
to form keratin
Cause
These
tumours often arise in skin damaged by long-term ultraviolet radiation and also
by X-rays and infrared rays. Other carcinogens include pitch, tar, mineral oils
and inorganic arsenic (see Basal cell carci-noma). Certain rare genetic
disorders, with defective DNA repair mechanisms, such as xeroderma
pigmen-tosum, lead to multiple squamous and basal cell carcinomas, and to
malignant melanoma; this illustrates the importance of altered DNA in the
pathogenesis of malignancy. The DNA of the human papilloma virus can be integrated into the nuclear DNA of
keratinocytes and cause malignant transformation. Immunosuppression and
ultraviolet radiation predispose to this.
Multiple
self-healing squamous cell carcinomas are found in the autosomal dominant trait
described by Ferguson-Smith. The abnormal gene lies on chromo-some 9q.
Clinical presentation and course
Tumours
may arise as thickenings in an actinic ker-atosis or, de novo,
as small scaling nodules; rapidly growing anaplastic lesions may start as
ulcers with a granulating base and an indurated edge (Fig. 18.36). Squamous
cell carcinomas are common on the lower lip (Fig. 13.36) and in the mouth.
Tumours arising in areas of previous X-radiation or thermal injury, chronic
draining sinuses, chronic ulcers, chronic inflammation or Bowen’s disease are
the most likely to metastasize. Tumours arising in non-exposed sites, such as
the perineum and sole of foot and on the ear and lip, have a lesser malignant
potential but may metastasize. Squamous cell carcinomas arising in sun-exposed
areas and in actinic keratoses seldom metastasize. Tumours more than 2 cm in
diameter are twice as likely to recur and metastasize compared with smaller
tumours. Metastatic potential is also high in tumours greater than 4 mm in
depth or invad-ing to the subcutaneous tissue, in poorly differentiated
tumours; in tumours with perineural involvement; and in those arising in the
immunosuppressed.

Histology
Keratinocytes disrupt the dermo-epidermal junction and proliferate irregularly into the dermis. Malignant cells usually retain the capacity to produce keratin (Fig. 18.37).
Treatment
After
the diagnosis has been confirmed by biopsy, the tumour should be excised with a
0.5-cm border of normal skin. Mohs’ micrographic surgery is useful for
high-risk tumours. Radiotherapy is effective but should be reserved for the
frail and the elderly.
Related Topics