Morphology, Culture, Pathogenesis, Laboratory Diagnosis, Treatment and Preventive Measure - Treponema Pallidum | 12th Microbiology : Chapter 7 : Medical Bacteriology
Chapter: 12th Microbiology : Chapter 7 : Medical Bacteriology
Treponema Pallidum
Treponema Pallidum
Treponema pallidum is
included in the family Spirochaetaceae. They are slender
spirochaetes with fine spirals having pointed ends. Some of them are pathogenic
for humans, while others are normal flora in mouth and genitalia. These
pathogens are strict parasites and the diseases caused by Treponema are called
Treponematoses. Treponema pallidum is the causative agent of
syphilis. The name Treponema pallidum is derived from Greek words, which means, Trepos Turn Nema –Thread and Pallidum
– Pale staining.
Morphology
It is
thin, delicate spirochete with tapering ends, about 10µm long and 0.1–0.2 µm
wide. It has about ten regular spirals, which are sharp and angular, at regular
intervals of about 1µm. They are actively motile (endoflagella), exhibiting
rotation around the long axis, backward and forward movements and flexion of
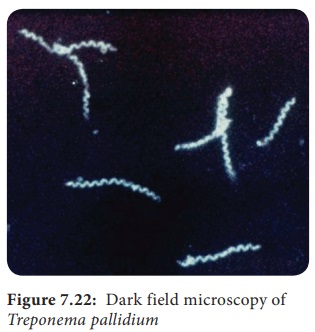
the whole body. It cannot be seen under light microscope and does not take ordinary
bacterial stains. It can be seen under the dark ground (Figure 7.22) or phase
contrast microscope. It can be stained by silver impregnation method.
Culture
• Pathogenic
Treponema cannot be grown in artificial culture media.
• Treponema pallidum strains (Nichol’s strain) are maintained in rabbit testes.
Pathogenesis
Source of
infection – Human beings (patients)
Mode of
transmission – Sexual contact Site of entry – Through minute abrasions/ cuts on
skin or mucosa
Incubation period – 10–90 days
• Treponema
pallidum causes venereal syphilis,
which is acquired by sexual contact. The pathogen enters the human body through
cut on the skin or mucosa of genital areas.
• The
clinical disease sets in after an incubation period of about a month. There are
3 clinical stage of venereal syphilis, namely – primary, secondary and tertiary
syphilis
Primary syphilis
• A papule appears on the genital area that
ulcerates, forming a chancre of primary syphilis called hard chancre.
• The chancre is covered by thick exudates, very
rich in spirochetes.
• The regional lymph nodes are swollen, discrete,
rubbery and non – tender.
• Even before the chancre appears, the spirochetes
spread from the site of entry into the lymph and bloodstream, so the patient may
be infectious during the late incubation period.
• The
chancre invariably heals within 10–40 days, even without treatment, leaving a
thin scar.
Secondary syphilis
• Secondary syphilis sets in 1–3 months after the
primary lesion heals. During this interval, the patient is asymptomatic.
• The secondary lesions are due to widespread
multiplication of the spirochetes and dissemination through the blood.
• Secondary syphilis is characterized by appearance
of papular skin rashes, mucous patches in the oropharynx and condylomata (a
raised growth on the skin resembling a wart).
• The lesions are abundant in spirochetes and the
patient is most infectious during the secondary stage.
• There may be retinitis (inflammation of the
retina of the eye), meningitis, periostitis, and arthritis.
• Secondary lesions usually undergo spontaneous
healing, in some cases taking as long as 4 or 5 years.
• After
the secondary lesions disappear, there is a period of dormant known as latent syphilis the patient does not
show any clinical symptoms but with positive serology.
Tertiary syphilis
• After several years, manifestations of tertiary
syphilis appear. These consist of cardiovascular lesions including aneurysms
(enlargement of an artery), gummata (a small rubbery granuloma that has a
necrotic centre) and meningovascular manifestations. Tertiary lesions contain
few spirochetes.
• In few
cases, neurosyphilis such as tabesdorsalis or general paralysis of the insane
develops. These are known as late tertiary or quaternary syphilis.
Congenital syphilis
In
congenital syphilis, the infection is transmitted from mother to fetus by
crossing the placental barrier.
Non – Venereal syphilis
It may
occur in doctors or nurses due to contact with patients lesion during
examination. The primary chancre occurs usually on the fingers.
Laboratory Diagnosis
The
diagnosis of syphilis includes
a. Demonstration
of Treponemes
b. Serological
tests
Specimen: Exudates are collected from the chancre. Blood (serum) is collected for serology.
Demonstration of Treponemes
a. Dark ground microscopy: The wet
film is prepared with exudates and
examined under dark ground microscope. Under dark field examination Treponema pallidum appears motile spiral
organism.
b. Treponemes in tissues: It can
be demonstrated by silver impregnation method of staining
Serological tests
Non –
Treponemal tests – In the standard tests for syphilis includes;
a. VDRL –
Venereal Diseases Research Laboratory test.
b. RPR –
Rapid Plasma Reagain (Figure 7.23).
VDRL or
RPR tests are used for serological screening for syphilis and more useful for
the assessment of cure following treatment.
TRUST – Toluidine red unheated serum test, modified form of RPR
test.
Treponemal Tests: The
treponemal tests includes
a. TPHA – Treponema pallidum hemagglutination assay
b. FTA –ABS – Fluorescent treponemal antibody
absorption test.
These two tests are used to confirm the diagnosis
Treatment and Preventive Measure
In early syphilis
a. Benzathine
benzyl penicillin,24 lakhs units intramuscularly in a single dose.
b. Alternatively,
doxycycline 100 mgtwice a day orally for 15 days
In late syphilis
Benzathine
benzyl penicillin 24 lakhs units, intramuscularly once weekly for 3 weeks.
• Avoiding
sexual contact with an infected individual.
• Use of sex
barriers (condoms).
Related Topics