Morphology, Cultural Characteristics, Antigenic Structure, Pathogenesis, Laboratory Diagnosis, Treatment - Streptococcus Pyogenes (Flesh eating Bacteria) | 12th Microbiology : Chapter 7 : Medical Bacteriology
Chapter: 12th Microbiology : Chapter 7 : Medical Bacteriology
Streptococcus Pyogenes (Flesh eating Bacteria)
Streptococcus Pyogenes (Flesh eating
Bacteria)
The genus
Streptococcus includes a large and
varied group of bacteria. They inhabit various sites, notably the upper
respiratory tract. However, some species of which Streptococcus pyogenes is the most important and are highly
pathogenic. The name Streptococcus is
derived from Greek word ‘Streptos’ which means twisted or
coiled.
Morphology
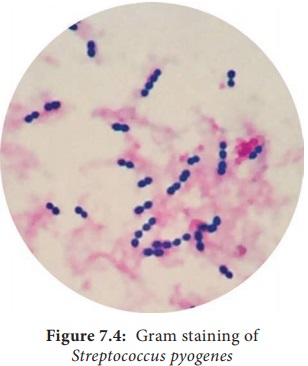
• They
are Gram positive, spherical or oval cocci and arranged in chains (0.6µm–1µm)
• They
are non – motile, non – sporing. Some strains are capsulated (Figure 7.4).
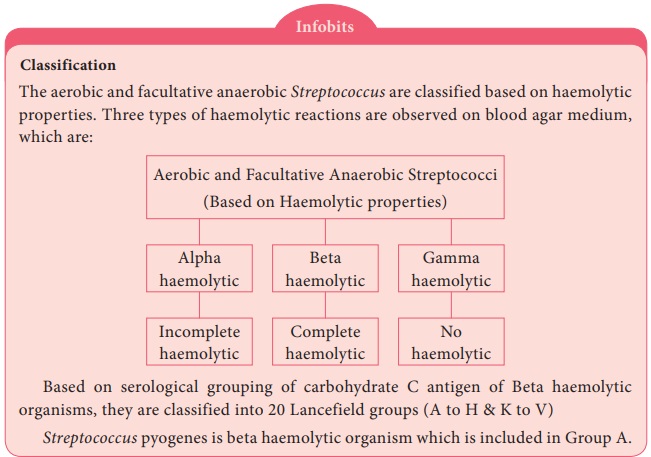
Cultural Characteristics
• They are aerobe and facultative anaerobe. Optimum
temperature is 37°C and pH is 7.4 to 7.6
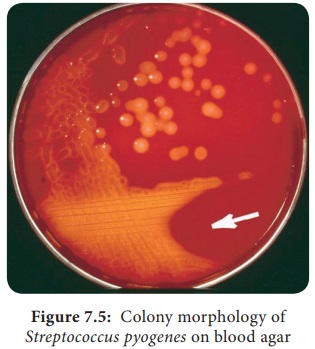
• They grow only in media enriched with blood or
serum. It is cultivated on blood agar. On blood agar, the colonies are small,
circular, semitransparent, low convex, with an area of clear hemolysis around
colonies (Figure 7.5).
• Crystal
violet blood agar – a selective medium for Streptococcus
pyogenes.

Antigenic Structure
Capsule: It inhibits phagocytosis
Cell wall: The outer layer of cell wall consists of protein and lipoteichoic acid which helps in
attachment to the host cell. Middle layer of cell wall consists of Group
Specific C – Carbohydrate that is used for Lancefield grouping. Inner layer of
cell wall is made up of peptidoglycan which has pyrogenic and thrombolytic
activity
Toxins and Enzymes: Streptococcus pyogenes produces
several exotoxins and enzymes which
contribute to its virulence.
Toxins and Hemolysins: Streptococci produces
two types of hemolysins which are Streptolysin O and Streptolysin S.
Erythrogenic toxin: (Pyrogenic
exotoxin) - The induction of fever is the primary effect of this toxin and it
is responsible for the rash of scarlet fever.
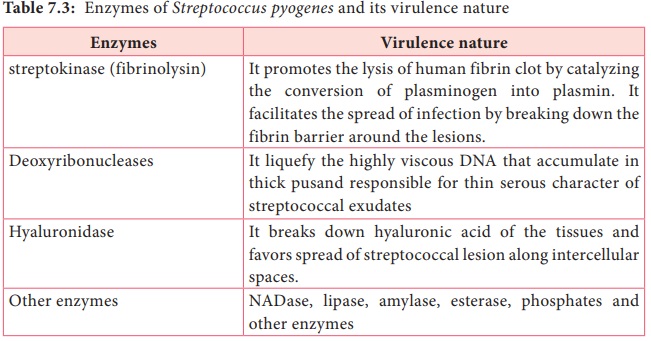
Enzymes: The various enzyme of Streptococcus pyogeneswhich
exhibits virulence activity are
listed in Table 7.3
Table
7.3: Enzymes of Streptococcus pyogenes and its virulence nature
Enzymes: Virulence nature
streptokinase (fibrinolysin): It
promotes the lysis of human fibrin clot by catalyzing the conversion of
plasminogen into plasmin. It facilitates the spread of infection by breaking
down the fibrin barrier around the lesions.
Deoxyribonucleases: It
liquefy the highly viscous DNA that accumulate in thick pusand responsible for
thin serous character of streptococcal exudates
Hyaluronidase: It breaks down hyaluronic acid
of the tissues and favors spread of streptococcal lesion along intercellular
spaces.
Other enzymes: NADase, lipase, amylase,
esterase, phosphates and other enzymes
Streptokinase: It is given intravenously for the treatment of early
myocardial infarction and other thromboembolic disorders. Streptococcus
equisimilis is the source of streptokinase used for thrombolytic therapy in
patients
Pathogenesis
Streptococcus pyogenes is
intrinsically a much more dangerous
pathogen than Staphylococcus aureus
and has a much greater tendency to spread in the tissues.
Mode of transmission: Streptococcal infections are transmitted by the
following ways:
Streptococcal diseases may be broadly
classified, and it is shown in flowchart 7.1
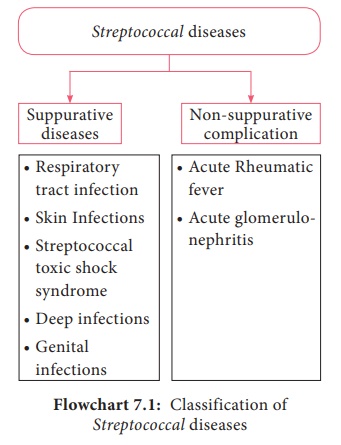
Suppurative Infections
1. Respiratory tract infection
a. Streptococcal sore throat: Sore
throat (acute tonsillitis and
pharyngitis) is the most common streptococcal diseases. Tonsillitis is more
common in older children and adults. The pathogen may spread from throat to the
surrounding tissues leading to suppurative (pus – formation) complication such
as cervical adenitis (inflammation of a lymph node in the neck) otitis media
(inflammation of middle ear), quinsy (ulcers of tonsils) Ludwig’s angina
(purulent inflammation around the sub maxillary glands) mastoiditis (inflammation
of mastoid process).
b. Scarlet fever: The
disease consists of combination of
sore throat and a generalized erythematous (redness of skin or mucous
membranes) rash..
2. Skin infections
a. Erysipeals: It is an acute spreading lesion. The skin shows massive brawny
oedema with erythema it is seen in elderly persons or elders.
b. Impetigo: (Streptococcal pyoderma)
It is a
skin infection that occurs most often in young children. It consists of
superficial blisters that break down and eroded areas whose surface is covered
with pus. It is the main cause leading to acute glomerulonephritis in children.
c. Necrotizing fasciitis: It is an
invasive, infection characterized by
inflammation and necrosis of the skin, subcutaneous fat and fascia. It is a
life-threatening infection
The strain which cause necrotizing fasciitis to have been named as
“Flesh eating bacteria or” killer bacteria.
3. Streptococcal toxic shock syndrome
Streptococcal
pyrogenic exotoxin leads to streptococcal toxic shock syndrome (TSS). It is a
condition in which the entire organ system collapses, leading to death.
4. Genital infections
Streptococcus pyogenes is an
important cause of puerperal sepsis
or child bed fever (infection occur when bacteria infect the uterus following
child birth)
5. Deep infection
Streptococcus pyogenes may cause pyaemia (blood poisoning characterized
by pus forming pathogens in the blood) septicemia (A condition in which
bacteria circulate and actively multiply in the bloodstream) abscess in
internal organs such as brain, lung, liver and kidney.
Non – Suppurative Complication
Streptococcus pyogenes infections
are sometimes followed by two
important non – suppurative complications which are, acute rheumatic fever and
acute glomerulonephritis. These complications occur 1–4 weeks after the acute
infection and it is believed to be the result of hypersensitivity to some
streptococcal components
1. Rheumatic fever
It is
often preceded by sore throat and most serious complication of haemolytic
streptococcal infection. The mechanism by which Streptococci produce rheumatic fever is still not clear. A common
cross reacting antigen exist in some group A streptococci and heart, therefore,
antibodies produced in response to the. streptococcal infection could cross
react with myocardial and heart valve tissue, causing cellular destruction
2. Acute glomerulonephritis
It is
often preceded by the skin infection. It is caused by only a few “nephritogenic
types (strains)”. It develops because some components of glomerular basement
membrane are antigenically similar to the cell membranes of nephritogenic
streptococci. The antibodies Formed against Streptococci
cross react with glomerular basement membrane and damage. Some patients develop
chronic glomerulonephritis with ultimate kidney failure.
HOTS: Why are some staphylococcal skin infections similar to
streptococcal skin infection?
Laboratory Diagnosis
Specimens: Clinical specimens are collected according to the site of lesion. Throat swab, pus or
blood is obtained for culture and serum for serology.
Direct Microscopy: Gram
stained smears of clinical specimens
is done, where Gram positive cocci in chains were observed. It is indicative of
streptococcal infection.
Culture: The clinical specimen is inoculated on blood agar medium and incubated at 37° C for 18–24
hours. After incubation period, blood agar medium was observed for zone of beta
– haemolysis around colonies.
Catalase test: Streptococci are catalase
negative which is an important test to differentiate Streptococci fromStaphylococci.
Serology: Serological tests are done for rheumatic fever and glomerulonephritis. It is established by
demonstrating high levels of antibody to streptococci toxins. The standard test
is antistreptolysin Otitration. ASOtitres higher than 200 units are indicative
of prior Streptococcal infection.
Treatment and Prophylaxis
• Penicillin G is the drug of choice
• In patients allergic to penicillin, erythromycin
or cephalexin is used.
• Antibiotics have no effect on established
glomerulonephritis and rheumatic fever.
• Prophylaxis is indicated only in the prevention
of rheumatic fever, it prevents streptococcal reinjection and further damage to
the heart.
• Penicillin is given for a long period in children
who have developed early signs of rheumatic fever
Myth: Eating choc-. olate encourages the
development of acne.
Fact: It is the oils and fats in many
chocolate products, and not chocolate itself, that promote sebum production and
subsequent acne. Chocolate in low-fat chocolate milk and in fat-free chocolate
candies does not encourage acne. Acne suffers do not need to give up chocolate,
they need to reduce their lipid consumption.
Related Topics