Chapter: Clinical Dermatology: The skin in systemic disease
The skin and diabetes mellitus
The skin
and diabetes mellitus
The
following are more common in those with dia-betes than in others.
1 Necrobiosis lipoidica.
Less than 1% of diabeticshave necrobiosis, but most patients with necrobiosis

The remaining few should have a glucose tolerance test followed
by regular urine tests as some will become diabetic later. The lesions appear
as one or more discoloured areas on the fronts of the shins (Fig. 19.3); they
are shiny, atrophic and brown-red or slightly yellow. The underlying blood
vessels are easily seen through the atrophic skin and the mar-gin may be
erythematous or violet. Minor knocks can lead to slow-healing ulcers; biopsy
can do the same. No treatment is reliably helpful.
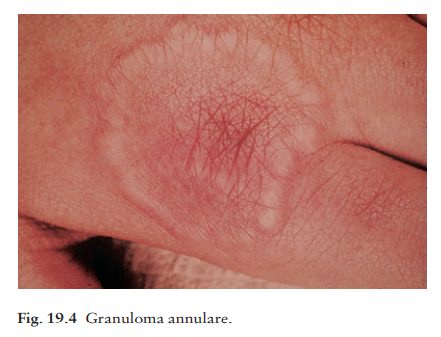
2 Granuloma annulare. The cause of granulomaannulare is not known and dermatologists still debate whether or not there is a genuine association with diabetes. If it exists at all, the association applies only to a few adults with extensive lesions. Children with standard lesions on the hands may need a single urine check for sugar but no more elaborate tests. Clinically, the lesions of granuloma annulare often lie over the knuckles and are composed of dermal nodules fused into a rough ring shape (Fig. 19.4). On the hands the lesions are skin-coloured or slightly pink; elsewhere a purple colour may be seen. Although a biopsy is seldom necessary, the histology shows a diagnostic palisading granuloma, like that of necro-biosis lipoidica. Lesions tend to go away over the course of a year or two. Stubborn ones respond to intralesional triamcinolone injections.
3 Diabetic
dermopathy. In about 50% of Type I dia-betics, multiple small (0.5–1
cm in diameter) slightly sunken brownish scars can be found on the limbs, most
obviously over the shins.
4
Candidal
infections.
5
Staphylococcal
infections.
6
Vitiligo.
7
Eruptive
xanthomas.
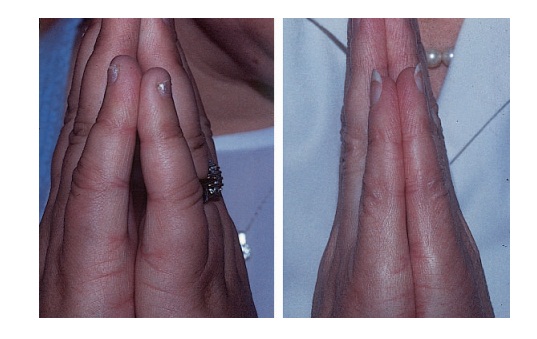
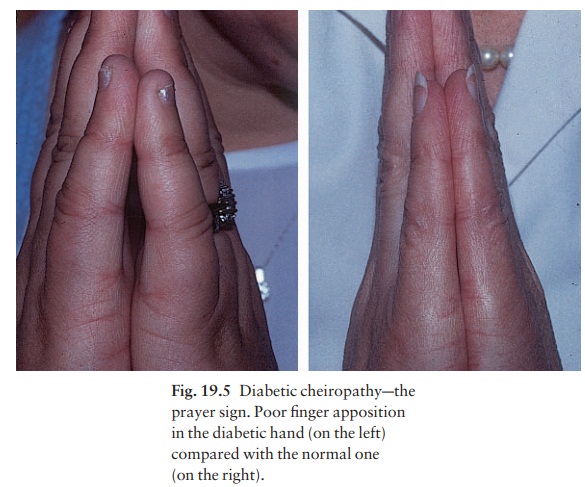
8 Stiff thick skin(diabetic
sclerodactyly or cheiro-arthropathy) on the fingers and hands, demonstrated by
the ‘prayer sign’ in which the fingers and palms cannot be opposed properly
(Fig. 19.5).
9
Atherosclerosiswith
ischaemia or gangrene of feet.
10
Neuropathic
foot ulcers.
Related Topics