Chapter: Clinical Dermatology: The skin in systemic disease
The porphyrias
The porphyrias
There
are at least seven enzymes in the metabolic pathway that leads to the synthesis
of haem. There are also seven different types of porphyria, each being caused
by a deficiency of one of these enzymes, and each having its own characteristic
pattern of accumu-lation of porphyrin and porphyrin precursors. Some of these
cause the photosensitivity (to ultraviolet radi-ation of wavelength 400 nm,
which is capable of pen-etrating through window glass) that is the cardinal
feature of the cutaneous porphyrias.
The different types can be separated on clinical grounds, aided by the biochemical investigation of urine, faeces and blood. Only five varieties will be mentioned here.
Congenital erythropoietic porphyria
This
is very rare, caused by mutations in the uropor-phyrinogen cosynthase gene, and
inherited as an auto-somal recessive trait. Severe photosensitivity is noted
soon after birth, and leads to blistering, scarring and mutilation of the
exposed parts, which become increasingly hairy. The urine is pink and the teeth
are brown, although fluorescing red under Wood’s light. A haemolytic anaemia is
present. Treatment is un-satisfactory but must include protection from, and
avoidance of, sunlight. Gene therapy may be possible in the future. The hairy
appearance, discoloured teeth and the tendency to avoid daylight may have given
rise to legends about werewolves
Erythrohepatic protoporphyria (erythropoietic protoporphyria)
In
this more common, autosomal dominant condition, caused by mutations in the
ferrochelatase gene, a less severe photosensitivity develops during childhood.
A burning sensation occurs within minutes of exposure to sunlight. Soon the
skin becomes swollen and crusted vesicles sometimes appear, leading to pitted
scars. Liver disease and gallstones occur. In addition to sun avoidance and the
use of sunscreens, beta-carotene may be given orally.
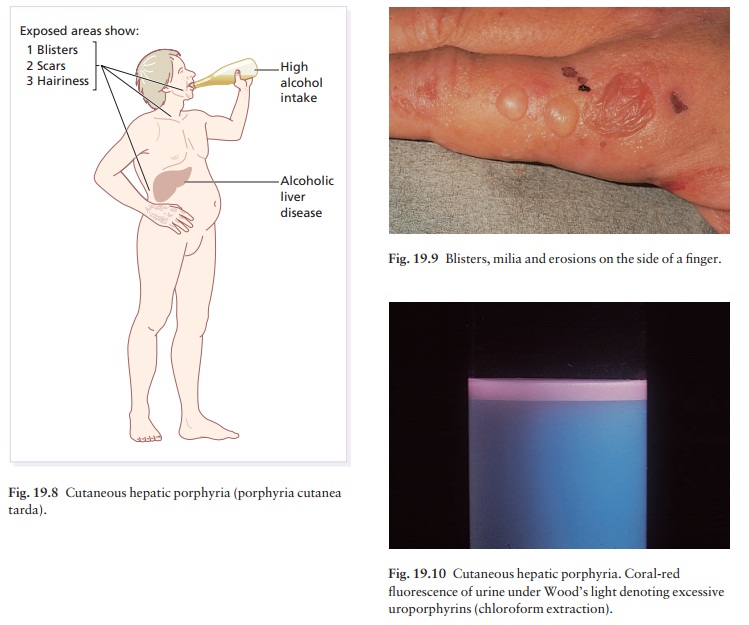
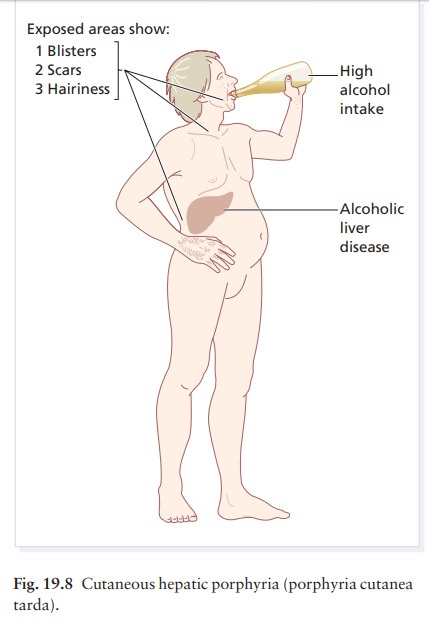
Cutaneous hepatic porphyria (porphyria cutanea tarda)
There are two types: a sporadic type (accounting for 80% of cases) and a type inherited as an autosomal dominant trait (20%). Both are characterized by low hepatic uroporphyrinogen decarboxylase activity.
The sporadic type is usually seen in men, but rarely in
women, who have damaged their livers by drinking too much alcohol but may also
occur in women taking oestrogens. Recently it has been shown that some cases
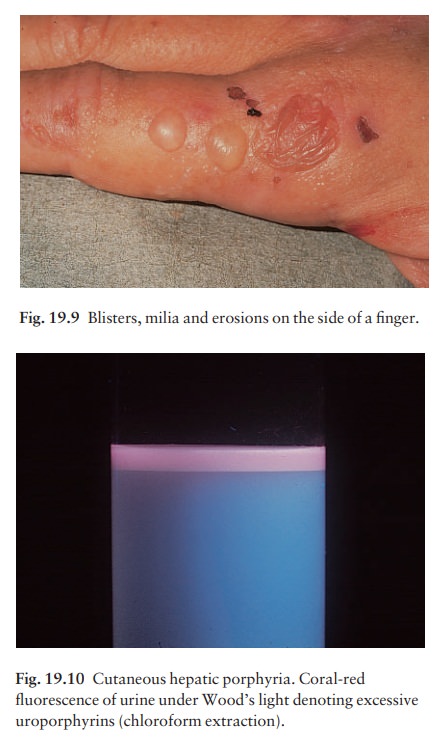
are caused by a previous hepatitis C virus infection. Blisters, erosions and milia
form on the exposed parts of the face, and on the backs of the hands (Figs 19.8
and 19.9), in response to sunlight or to minor trauma. These areas become
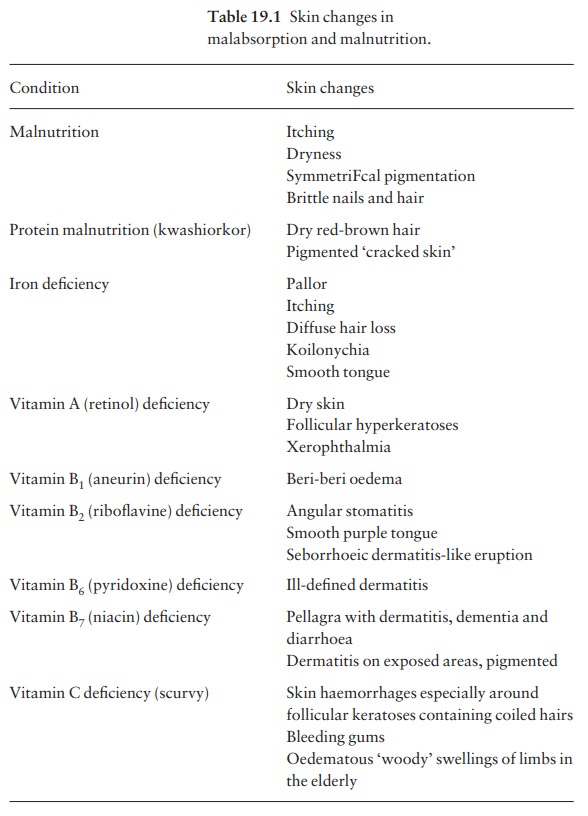
scarred and hairy. The urine is pink and fluoresces a bright coral-pink under
Wood’s light as a result of excessive
uroporphyrins (Fig. 19.10). Treatment is based on avoiding alcohol and
oestrogens, but other measures are usually needed too, including regular
venesection or very low-dose hydroxychloroquine therapy (e.g. 100 mg twice
weekly) under specialist supervision. Higher doses cause toxic hepatitis in
these patients.
Acute intermittent porphyria
This
condition, inherited as an autosomal dominant trait as a result of mutations of
the porphobilinogen deaminase gene, is most common in Scandinavia. Skin lesions
do not occur. Attacks of abdominal pain, accompanied by neuropsychiatric
symptoms and the passage of dark urine, are sometimes triggered by drugs
(especially barbiturates, griseofulvin, oestrogens and sulphonamides).
Variegate porphyria
This
disorder, inherited as an autosomal dominant trait, and a result of mutations
of the protopor-phyrinogen oxidase gene, is particularly common in South
Africa. It shares the skin features of porphyria cutanea tarda and the systemic
symptoms and drug provocation of acute intermittent porphyria.
Pseudoporphyria’
This
term is used when skin changes like those of cutan-eous hepatic porphyria occur
without an underlying abnormality of porphyrin metabolism. It is seen in a few
patients on haemodialysis, and can be induced by some drugsanotably frusemide
(furosemide) and non steroidal anti-inflammatory drugs. The overuse of sun beds
is another possible cause.
Related Topics