Chapter: Essential Anesthesia From Science to Practice : Applied physiology and pharmacology : Anesthesia and the lung
Spirometry
Spirometry
Pulmonary function tests (PFTs) are rarely indicated in preparation for anes-thesia, though they can tell us whether a patient with severe lung disease has been optimally prepared. Pulmonary restrictive and obstructive diseases worry us. Short of treating infection, we cannot do much about restrictive disease; how-ever, it can co-exist with obstructive bronchospasm, which is common and can be treated with bronchodilators. Of the many pulmonary function studies, we pay particular attention to forced vital capacity (FVC). FVC values below 15 mL/kg give rise to great concern. How much the patient can exhale in 1 second (FEV1), and whether this can be improved by bronchodilators determines obstructive
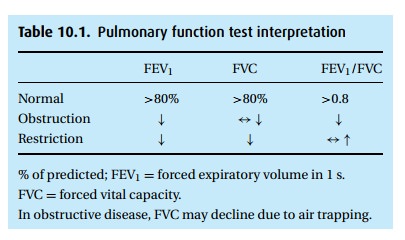
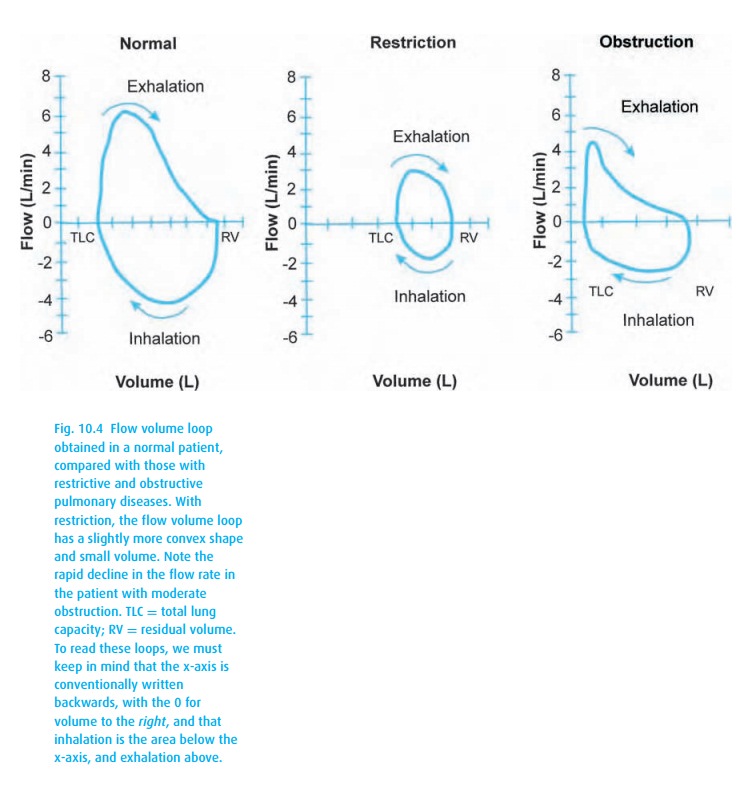
Typically, PFT results are reported as “% of predicted,” based on popula-tion studies that consider the patient’s height, age, and gender. We accept values of at least 80% predicted as normal. With obstructive disease, the patient exper-iences airway closure during exhalation, measured as a low FEV1 (Table 10.1). With advanced disease and air trapping, the FVC might also decline, though not as much as the FEV1, thus the hallmark of obstructive disease is a reduced ratio of FEV1 to FVC. With age, this ratio declines as well (to perhaps 0.7), so again we look at the percentage predicted. Flow volume loops (Fig. 10.4) can also be helpful.
Related Topics